COVID-19 pandemic has exacerbated systemic inequities rooted in ageism, ableism, classism, racism, sexism, etc. Shutdowns, physical distancing and wearing earplugs have allowed time, space and relative quiet to reflect on advocating for something better than normal (status quo).

According to San Francisco Department of Public Health (SF DPH) COVID-19 data tracker to date: 31,111 positive cases and 324 deaths (60.8% male; 61% age 80+, 16% age 70-79, 12% age 60-69, or 89% of deaths age 60+; 36.7% Asian, 20.1% Latinx, 28.4% White, 8.3% Black; 0.6% homeless). Total COVID-19 deaths: 442,951 in U.S., over 2.18 million worldwide.
SF appears to have peaked at 373 new COVID-19 cases on Jan. 8. After surges from holidays and ongoing attempts to recall Governor, California lifted stay-at-home orders so SF will return to limited re-openings…until the next surge, especially with more contagious coronavirus variants spreading?!

Looks like SF DPH Director Grant Colfax is modeling layered masks for extra protection on Jan. 25? This is first press conference where he did not remove his mask! SF DPH’s latest Stay Safer at Home order (Jan. 27) is 99 pages…for bedtime reading!

Early in COVID pandemic, SF DPH prioritized “equity” to protect more vulnerable groups based on age (older), race (Latinx, Black), socio-economic (unhoused, living in crowded housing, without health insurance coverage), etc. Given these diverse interests, the pandemic response has been fraught with mixed messages and shifting priorities.
To its
credit, SF DPH shifted to coordinate outreach with trusted members of these impacted
communities, COVID-19 testing free at City sites (though when supply ran low, insured people told to get tested through private providers so City sites could serve
uninsured), vaccine notification sign-up via text/email for people with
smartphone/internet access, and now creating vaccination sites to serve anyone
eligible to receive free vaccines. Most sites are set-up to meet people
where they are, including near public transit stops and allowing walk-ups and
drive-through at high-volume sites.

In SF, gender gap in COVID-19 cases appears to be narrowing, though men still die at a higher rate that could be related to their higher prevalence of autoantibodies, high-risk behaviors, occupational exposure, etc.

On Jan. 6 noon launch of California’s Master Plan for Aging (MPA), California Health & Human Services Secretary Mark Ghaly (pediatrician) lauded older adults as “heroes” for their “leadership” and “sacrifices”—stay at home, save lives—during COVID-19 pandemic.
Gag the “hero” narrative; even health care workers reject “hero” label, as martyrdom against their will, sacrificed by failures to supply PPE. Older adults under lockdown in residential long-term care (LTC) facilities (like prisoners) were stripped of their self-determination, while non-institutionalized SF residents of all ages were “followers” (not leaders) of SF’s Stay Safer at Home order and extensive lockdowns that limited movement outside home to “essential activities.”

What are shut-ins doing at home? Before pandemic, older adults age 65+ watched TV for average of 4.5 hours per day; during pandemic, TV watching surged 8 hours a week per household and 35% increase in streaming video consumption.

Fernando Gil-Torres, UCLA Director for Center of Policy Research on Aging, presented on California’s changing demographics: living longer at 81.9 years, California has 2nd highest average life expectancy in the nation (after Hawaii)! And California’s older population is becoming more racially/ethnically diverse; within 10 years, non-Hispanic whites will no longer represent the majority of older adults.

Jennie Chin-Hansen, former CEO of On Lok and American Geriatrics Society, introduced California MPA’s 5 Bold Goals, with equity “baked in” each, for 2030:
#1 Housing
for All Ages and Stages: live where we choose as we age in communities that
are age-, disability-, and dementia-friendly and climate- and
disaster-ready. Target: Millions of New
Housing Options to Age Well
#2 Health
Reimagined: access to services we need to live at home in our communities
and to optimize our health and quality of life.
Target: Close the Equity Gap in and Increase Life Expectancy
#3 Inclusion
and Equity, Not Isolation: lifelong
opportunities for work, volunteering, engagement, and leadership; protection
from isolation, discrimination, abuse, neglect, and exploitation. Target: Keep Increasing Life Satisfaction as
We Age
#4 Caregiving
That Works: prepare for and support
through rewards and challenges of caring for aging loved ones. Target: One Million High-Quality Caregiving
Jobs
#5 Affording
Aging: economic security for as long as we live. Target: Close the Equity Gap in and Increase
Elder Economic Sufficiency

A week after MPA (45-page report) launch, California Department of Aging (CDA) Director Kim McCoy Wade went deeper into 10-year blueprint to promote Equity in Aging: California for All Ages by 2030! Yes, equity includes intergenerational component, explicitly calling for age-integrated community centers and volunteer engagement! MPA reports that California has more multigenerational households than any other state, due to housing costs and other financial constraints, care needs, and cultural preferences. (Yet, it doesn’t call for de-ghettoization of age segregation in housing.)
MPA is framed
around 5 goals (23 strategies, 100+ action-ready initiatives), Local Playbook, and Data Dashboard to track progress
in implementing MPA for accountability. State’s ten cabinet agencies in
partnership with federal government, private sector, community groups and all stakeholders
will launch 100+ initiatives within the first two years (2021-2022)!

Why on earth did CDA illustrate MPA Goal 1: Housing for All Ages & Stages with steps leading to front door entrances of houses and overgrown foliage on sidewalk? How age- and disability-friendly is this design for people who use wheelchairs or walkers, and/or depend on door-to-door paratransit? Possibly disaster-ready for earthquakes if wood-frame houses can lean on each other for support? Focus on aging in place, not constructing more segregated age 55+ communities.
Two days
after launch of MPA, Governor’s proposed budget included $250 million toward
buying or rehabilitating assisted living facilities for low-income seniors. 
COVID-19 is upending MPA Goal 2: Health Reimagined by closing equity gap and increasing life expectancy. Due to COVID-19 pandemic deaths last year, life expectancy at birth for Americans will shorten by 1.13 years to 77.48 years—the largest single-year decline in life expectancy in at least 40 years and is the lowest life expectancy estimated since 2003. Researchers from University of Southern California and Princeton estimated life expectancy declines for Black and Latinx that are 3-4 times that for Whites, widening racial disparities in life expectancy.
·
Whites
77.84 (decline by 0.68 years)
·
Blacks
72.78 (decline by 2.10 years)
·
Latinx
78.77 (decline by 3.05 years)
Asians, with life expectancy of 86.67 years, not included in research.
“Of
all the forms of inequality, injustice in health care is the most
shocking and inhumane.”—Martin Luther King, Jr. speech to Medical Committee for
Human Rights (Mar. 25, 1966)
California’s older adults age 65+ make up 10% of state’s population, and 75% of COVID-19 deaths during pandemic. MPA reported only 2% of California’s population live in nursing homes, but accounted for a third of COVID-19 deaths. COVID-19 death toll is inhumane, and the underreporting of deaths a grave injustice to lives lost (particularly in New York, where its Governor ordered nursing homes to admit recovering COVID-19 patients while granting immunity to providers, and his subsequent cover-up in undercounting nursing home deaths by as much as 50%)!

One reason for life expectancy gap is scientific racism and medical apartheid, according to Donald Moore, MD, MPH, of Physicians for a National Health Program-NY Metro, in a virtual forum on systemic racism in medicine, Unequal Treatment: The Unjust Death of Dr. Susan Moore. He moderated a panel calling for greater representation of Blacks in medical field, against closure of Black medical schools while other medical schools didn’t admit Blacks, for affirmative action (though Blacks have not benefited as much as women), against Kaiser Permanente Medical School (Pasadena) firing Black Dr. Aysha Khoury after she taught a class on racial health disparities last summer, etc. The curriculum in medical schools racialize disease, presuming Blacks have higher threshold for pain, training bias in future physicians “to minimize the pain, forgo the consent, blame the behaviors and dismiss the concerns of patients of color.”

In a video recorded from her hospital bed before she died of COVID-19 last month, 52-year-old Black internist Dr. Susan Moore described racist treatment by white physician who dismissed her complaints of pain and requests for medication at Indiana University Health. Camara Phyllis Jones, MD, MPH, PhD, family physician and epidemiologist, led conversation about dismantling systemic racism rooted in health care, asking: “Why is it that we as Black, Hispanic, Latino, Indigenous and marginalized people have to keep showing proof of our pain and oppression? The answer is not just racism. It is racism denial.”
The panelists discussed the importance of demanding institutional accountability in order to create substantial change, and reflected on how a publicly-financed single-payer system is a critical step in eradicating the racism that underpins inequities in our current health care system. This would be similar to how Medicare forced desegregation of hospitals by threatening to withhold federal funding from hospitals that practiced racial discrimination. (Dr. Susan Moore’s GoFundMe page set-up as she was sole provider to her surviving teenage son and her parents who both have dementia.)

Many rich intergenerational discussions to advance MPA Goal 3: Inclusion & Equity, Not Isolation: LGBT culture, age-friendly workplace, anti-racism, feminism, financial elder abuse prosecutions, and digital equity.

As part of CDA’s Ensuring Equity in Aging webinar series, this month focused on The Culture of LGBT Older Adults.

Jenny Pardini, Community Education Advocate at Legal Assistance for Seniors (Oakland), discussed why LGBT and other marginalized older adults are vulnerable, and what providers can do to ensure equity.

Jenny discussed importance of California AB 959, LGBT Disparities Reduction Act, on collecting data on SOGI (sexual orientation, gender identity) and more: if person identifies as transgender/non-binary, ask follow-up questions regarding preferred pronoun and preferred name; Queer is generally not preferred term for LGBT people who came of age prior to mid-1970s. (California SB 932 mandates reporting SOGI for COVID-19 deaths.) Without asking for SOGI, LGBT community risks being invisible/forgotten/erased.
When I inquire about SOGI, my cisgender
older clients appear confused and often respond, “I’m
normal!” (probing further, they mean heterosexual); some transgender clients
identify as transgender male/female and associated pronouns, but do not want
“transgender” documented in their charts; rare for older client to identify as
gender non-binary (they/them).
Jenny added that
Section 1557 of Affordable Care Act prohibits discrimination on basis of gender
identity (Medicare has specific code, condition 45, that tells system that
services are appropriate for particular person’s body parts; since May 2014, Medicare
may cover gender reassignment surgery based on medical necessity).

Karen Anderson of Lavender Seniors of East Bay provided LGBTQ History (today’s seniors grew up in a time when their SOGI was considered a mental/religious aberration; survived by being “closeted” and “passing” as heterosexual; experienced mental health/substance abuse issues from discrimination and self-imposed isolation, etc.) and how many older LGBTQ seniors still feel at risk from lifelong experiences of marginalization (increasing vulnerability with age, many avoid supportive services in desire to remain closeted, distrusting of institutions they may need in later life, more likely to be living alone without traditional family supports and planning for LTC needs, continuing discrimination in housing/LTC facilities, not having access to retirement benefits associated with marriage—though in 2017, Social Security Administration reopened decisions that denied spousal/survivor benefits to same-sex partners based on discriminatory marriage ban).

Karyn Skultety, Executive Director of Openhouse since 2017, presented on policy/advocacy: Because marginalized populations “age” faster due to trauma and poor access to social determinants of health due to discrimination, she recommended reconsidering age limits (65+) on senior care. For example, a senior designated Low Income Housing Tax Credit (LIHTC) community may provide for lower minimum age of 55 or 62.
Openhouse was founded in 1998 by psychologist Marcy
Adelman and her late partner Jeanette Gurevitch (1948-2002; SFSU MSW alum), to build
SF’s first LGBT+ welcoming senior (age 55+) affordable housing, with onsite
support services: 40 units at 55 Laguna (also home to
Bob Ross LGBT Senior Center) in 2017, with 68% residents identifying as LGBTQ; and
79 units at 95 Laguna in 2019, with 55% LGBTQ.
A week after
her presentation, Karyn announced that she was stepping down as Openhouse ED,
effective May 31, 2021, to prioritize family and return to her home state of Colorado.

"It ain't easy being surrounded by millennials in West Hollywood. I had the experience a few months ago — going up the street by a group of gay white men in their thirties. I heard one of them say, 'Let grandpa go by.' So as I passed, I said, 'Stay well, my grandchildren.' You’ve got to laugh." –Frank Galassi, age 82, on humor and vocabulary of happy aging, “Lessons on Resilience From LGBTQ Elders: Enduring hardship makes this population masters of perseverance,” Next Avenue (Jan. 6, 2021)

Monmouth University School of Social Work, New Jersey Foundation for Aging, and Lifelong Montclair hosted Ageism, -isms, and the Workforce in the Age of COVID-19 conference. Tim Driver, President of Age-Friendly Foundation, developed CAFÉ (Certified Age-Friendly Employer) as an employer-recognition program in 2006, using a proprietary evaluation method (12 standards listed above), to certify over 100+ employers (listed on website includes many financial, government, insurance, home care, retail, and telecommunications employers).

Charlotte Japp, CEO of CIRKEL, founded her intergenerational membership platform to connect generations for mutual personal and professional growth: Millennials like herself seek mentorship from Boomers like her parents who seek to stay relevant after being pushed out of their jobs at age 45. Charlotte walks the talk, moving back to her parents’ home in New York twice since graduating college!

Margaret Morganroth Gullette, author of Ending Ageism, or How Not to Shoot Old People (2017), talked about “middle ageism” starting at age 40, pandemic’s effect on job discrimination and unemployment during midlife, need for collective action to organize in a multi-generational coalition for new jobs and unionization that pulled up the middle-class. She was introduced by Rutgers Social Work Professor Lauren Snedeker, author of Strength in Numbers: A Millennial’s View on the Value of Working with Older Adults (2016).

In celebration of Martin Luther King, Jr. Day, Madam Walker Legacy Center and Indiana University (IU) presented A Call to Action: Then and Now, with activists Angela Davis (Silent Gen) and Alicia Garza (Millennial co-founder of #BlackLivesMatter), discussing "then" and "now" for civil rights, social justice, inclusion, and equality, to build a world more reflective of MLK, Jr.’s Dream.
Program
kicked off with pre-recorded welcome by IU President Michael McRobbie, who
announced measures to improve diversity, equity and inclusion consistent with
MLK, Jr. legacy; for example, IU School of Medicine (affiliated with IU
hospital where Dr. Moore received alleged racist treatment before her COVID-19
death) was awarded grant to help educate medical students to better care for
underserved populations. (Older adults are underserved, given
shortage of geriatricians!)

Angela Davis said MLK, Jr. legacy is a call for black freedom requiring radical changes in structures of society, in opposition to white supremacists who cling to past with confederate flags, MAGA and racial capitalism; need to defund police link to slavery/mass incarceration and imagine new institutions that do not rely on violence; strategies to bring BIPOC into institutions try to diversify but do not change systems that perpetuate racism. Examples: South Africa now has almost all-black police, but same problem of inflicting violence on POC embedded in system; not assume work is done after Black President Obama elected, but should have demonstrated against his deportations; Biden is moderate and needs to be pushed in struggle for revolution. (Will Biden's "diversity cabinet" appointees, which exclude Asian Americans, help marginalized people or perpetuate ruling class politics?)
She talked
about campaign to transform marginalized into mainstream, calling for universities
to stop marginalizing ethnic and feminist studies in curriculum, and need for
interdisciplinary studies. While she never
before had seen so many white participants in anti-racist protests against
police brutality after George Floyd was lynched, she voiced concern how radical
ideas get co-opted by status quo (capitalized by corporations) so need for more
radical ideas and collective activism to engage, organize, and mobilize more
people into fold demanding structural changes. She argued that because systems of injustice
and inequality faced by Black people were not created by Black people, they
cannot be dismantled by Black people; instead, white people need to recognize
their problem and their stake in the future of justice, equality and freedom as
anyone else.

Alicia Garza said racism is about rigged rules, with lots of “nice” people who help advance racist systems, show up at Jan. 6 U.S. Capitol insurrection (“inside job”) and resort to violence if they can’t control by consent, after Black voters helped secure victory in runoffs for 1st Black and 1st Jewish senators from Georgia (Warnock and Ossoff, who each raised more than $100 million to fund their campaigns) to return Democratic control of U.S. Senate, threatening white power structure. She called to transform how systems operate, hold government accountable, include people at the table and distribute resources in the richest country where there’s “plenty for everyone”!
Jan.
6 is a date that will live in infamy for launch of California’s first-ever MPA, which took place at noon Pacific Time
while white supremacists rioted the U.S. Capitol in Washington, D.C.! As I was absorbed attending the live MPA
program, I was clueless to the insurrection occurring real-time at our nation’s
capital. Great listening to this
intergenerational discussion about where to go from this current state of
affairs. In particular, can we advance more progressive policies to uplift all lives, instead of allowing authoritarian opportunists to use race and economic class anxiety that further divide people?

·
john
a. powell, director of Othering & Belonging Institute and contributor to Trumpism and Its Discontents (2020), believes rioters storming the Capitol was a
coup, particularly given the lack of police response, and Trump has channeled
rioters’ underlying white resentment (i.e., white people’s loss of status
translates to racial hostility).
·
Ian
Haney Lopez (“HaLo”), author of Merge Left: Fusing Race and Class, Winning Elections, and Saving America (2019), was not sure it was a coup; rather, he
believes Trumpism (“stoking racial fear to break solidarity culture wars”) has
been over 50 years in the making, in response to the success of the New Deal (government
work for majority v. very rich) with a faction of Republicans working for the rich
and, instead of appealing to class dynamics, promote propaganda that “civilized
white folks” are under threat of being replaced by “savage POC.” This has played out with police treating
protestors for racial equality as dangerous v. hands-off white resentment/rage
at Capitol. He urged us to learn more on
how to beat dog-whistle politics and build race-class solidarity at https://race-class-academy.com/: “When
we come together to reject racism as a weapon of the rich, we can make sure
that the government works for all of us, of every race and color.”
(HaLo’s thinking about multi-racial
shared power reminds me of how multi-ethnic Asian settlors organized in plantations of
Hawaii, building “local” solidarity.
HaLo, who attended Punahou and Harvard Law as contemporary of Deporter-in-Chief
Obama, believes racist call-out strategy doesn’t work, and Obama lacked
confidence to challenge racism but followed Clinton in new Democrat tradition
of getting funding from Wall Street and ruling on their behalf, like bailing
out banks during Great Recession.)

Shorenstein Center hosted wonderful intergenerational discussion of Beyond White Feminism: Not 'Healing' US Back to an Anti-Feminist Future with Koa Beck (Mills ’09), author of White Feminism: From the Suffragettes to Influencers and Who They Leave Behind (2021); Benita Roth, Binghamton Professor and author of Separate Roads to Feminism: Black, Chicana, and White Feminist Movements in America's Second Wave (2010); and Barbara Smith, activist who co-founded Combahee River Collective (which called attention to racism in feminist movement in 1974) and Kitchen Table: Women of Color Press (with Audre Lorde in 1980).
They discussed
ways that gender policies can be re-envisioned for a more inclusive future of
equity and opportunities rather than return to the old “normal” (exploitative
labor, poor wages, lack of paid and/or subsidized parental leave and family care); confronting white
supremacy, challenging systems of patriarchy and neoliberalism, defunding
police (stop militarizing poor communities of color and mass incarceration),
funding social safety net and Green New Deal, actively recruiting academics of
color and women in STEM, pushing for workers’ rights in addressing care crisis,
etc.
Last summer,
National Organization for Women (NOW) and Planned Parenthood NY (whose founder Margaret Sanger
promoted eugenics) finally woke to their own systemic racism and ousted their
white feminist leaders after complaints of racism and toxic “mean girl”
culture. Aileen Fernandez,
African-American who succeeded NOW founder Betty Friedan as President in
1970-71, resigned from NOW to focus on racial inequity; fifty years later, NOW
has a Black President again.

“The crime of financial abuse of elders is rampant and growing. People are living longer and they become more vulnerable with age. An older, perhaps forgetful person is an easy target. Why isn’t law enforcement going after the perpetrators?”—Carolyn Rosenblatt, “Frustration For Families: Law Enforcement Isn’t Pursuing Financial Elder Abusers,” Forbes (Sept. 27, 2019)
Paul Greenwood, retired San Diego elder abuse deputy district attorney
(DA), answered this question in Dissecting Elder Financial Exploitation: When
it’s Not Just a Civil Matter: sometimes determination
to pursue a case as civil v. criminal is made by police, who gather evidence
but typically are not qualified to interpret evidence using legal
analysis, which is the job of the prosecutor. For example, apparent
voluntariness is diluted by fraud, undue influence or exploiting mental limitations
of older victim—as in a case that police decided was civil until DA’s
investigator found evidence of fraudulent photo of suspect who photo-shopped
his image into couple’s portrait, suspect claimed to be long-lost nephew and persuaded
older woman to purchase property as joint tenants with his right of
survivorship; suspect sent to prison! Paul
emphasized importance of multi-disciplinary Financial Abuse Specialist Teams
(FAST).

During
the pandemic, which has hit older adults especially hard, this divide between
technology “haves” and “have-nots” has serious consequences.
Older adults in the “haves” group have more access to virtual social interactions and telehealth services, and more opportunities to secure essential supplies online. Meanwhile, the “have-nots” are at greater risk of social isolation, forgoing medical care and being without food or other necessary items.—Judith Graham, “Technology Divide Between Senior ‘Haves’ and ‘Have-Nots’ Roils Pandemic Response,” Kaiser Health News (July 24, 2020)
SF Tech
Council hosted Equity through Technology conversation with Google guys
on how they work with public sector organizations to find data-driven solutions
around issues of access and equity.
·
For
people with tech devices and internet access, they shared Grow with Google https://grow.google/, a free online training resource
intended to increase digital participation. (New Blogger makes me want to
decrease my participation☹.)
·
To
increase digitally accessible communication across “continuum of language,”
Google provides language translation, artificial intelligence virtual agents,
speech-text-speech https://speechtextspeech.appspot.com/, captioning, etc. Google also worked with State of Hawaii on
application that translates legislative content into 80 languages (but no
Pidgin, like Hawaiian Pidgin Bible). https://ets.hawaii.gov/ets-collaboration-with-google-cloud-leads-to-development-of-language-translation-application/
·
Examples
of using power of data for equitable service: look at communities most impacted
by COVID-19 and then gauge their willingness to receive vaccine; review google
search patterns to see waves of interest in varying topics (e.g., senior meals
related searches in April, testing sites in early May) that can inform need to
mobilize services

MPA Goal 4: Caregiving that Works has target of 1 million high-quality caregiving jobs. This is challenging given the history of gender and racial discrimination in caregiving work, with BIPOC women providing disproportionate share. Caregiving is also essential work that is often invisible as it takes place in institutions and private homes.

JFCS Seniors at Home hosted Caregiver: A Love Story (2020) documentary short film screening + discussion about family caregiver experience with filmmaker Jessica Zitter, MD, MPH (who previously made Extremis film about her work with ICU patients at end-of-life).
Dr. Zitter
intended to make a film about home hospice, which she arranged for her 59-year-old
friend Bambi, who decided to forgo further treatment for her terminal cancer
and live out her final weeks at home.
After Bambi’s husband Rick quit his job to become unpaid primary
caregiver during the last 9 weeks of Bambi’s life, Rick became ill himself and got
respite when Bambi goes to a nursing home for five days. (Respite in nursing
home not good option during pandemic! According to Rick, home hospice offered
only 1.5 hours of personal assistance per week, and they couldn’t afford to pay
for homecare.) After Bambi’s death, Rick said he had no regrets because “this
is all about love.”
While editing
the filmed footage, Dr. Zitter shifted focus to Rick as 24/7 caregiver, who
ends up assisting with toileting and more, though Bambi initially said she
never wanted him to “wipe my butt.” Mature,
modern and realistic love story…unlike sappy Love Story (1970) that
opens with “What can you say of a 25-year-old girl who dies?” (I say, call her a 25-year-old “woman”!)
JFCS Palliative Geriatric Care Manager Gwen Harris (SFSU MA Gerontology ‘06) moderated discussion with Dr. Zitter, who explained that as a palli doctor focused on patient care, she did not know about “family caregiver burden,” which she now considers a “rising public health crisis” and called for legislation to support family caregivers like Biden’s Plan.

MPA Goal 5: Affordable Aging targets closing equity gaps and increasing elder economic security. MPA noted local model: SF’s Project Homekey (plan for SF residents in emergency housing to exit into permanent supportive housing hotels purchased by the City using state grants) and Meals Expansion during COVID-19 pandemic.
To prevent
spread of coronavirus, California housed 22,300 people (including 2,000 in SF,
prioritizing seniors and adults who are medically vulnerable) under Project Roomkey. With Project’s cost of rooms
reimbursable from Federal Emergency Management Agency (FEMA)—only 75% under
Trump, and now increased to 100%, retroactive and continuing through September
2021 under Biden…SF plans to open more hotel rooms to house homeless! Much needed, as MPA
report points out that California residents age 50+ are the fastest growing
population of homeless in the state, and unhoused older adults experience health
problems typically seen in people 20 years older.
Recently, CDA
Director was appointed to California Department of Insurance’s LTC Insurance Task Force, charged with preparing a feasibility
report with recommendations by January 1, 2023 for a statewide LTC insurance
program intended to address inequities in affordable LTC within health and
social support systems.
COVID-19
vaccine eligibility priority groups
With
limited vaccine supplies, being classified as vulnerable is desirable for people
who seek vaccine prioritization.

This month’s Senior & Disability Action (SDA) meeting focused on setting this year’s advocacy priorities, with a review of last year’s successful care rationing campaign that could be used for vaccine prioritization.
1. What is our demand? Change state care
rationing guidelines – no discrimination against seniors and PWD
2. Who is target (who can make change)?
CA Governor, DPH Director
3. Who benefits? Constituents account for equity
4. Who’s with us? Allies
5. Who’s against us? Opponents
Last
month, CDC Advisory Committee on Immunization Practices (ACIP) recommended this
prioritization for offering COVID-19 vaccination:
·
Phase
1a, health care personnel and LTC facility residents
·
Phase
1b, persons aged ≥75 years (given high risk of hospitalization, illness and
death from COVID-19) and non–health care frontline essential workers (firefighters, police,
corrections, food & agri, US Postal Service, manufacturing, public transit,
teachers, daycare)
·
Phase
1c, to persons aged 65–74 years, persons aged 16–64 years with high-risk
medical conditions, and essential workers not included in Phase 1b.
After Phase 1a, states left to create own prioritization plans. On Jan. 12, federal government extended eligibility from age 75+ to 65+, and to people under age 65 with pre-existing health conditions to speed up process, though vaccine supply fell short. Next day, California opened vaccines to age 65+, but left out younger people with pre-existing conditions.
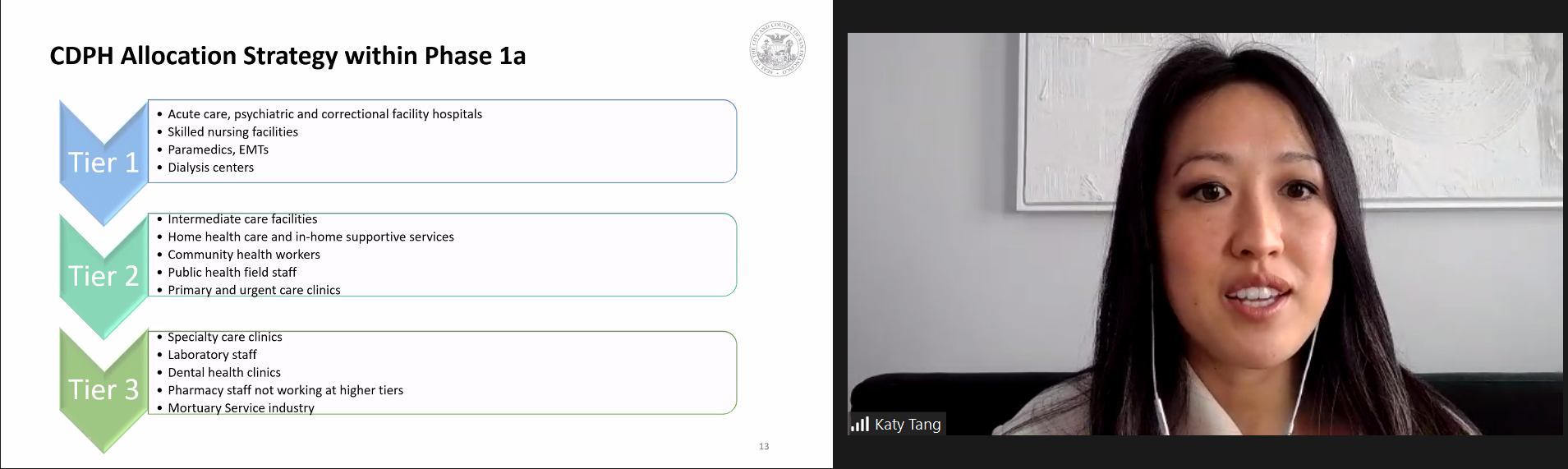
On Jan. 19, SDA’s Care Rationing Workgroup hosted forum on COVID Vaccination Allocation with Katy Tang, SF DPH Director of Public and Governmental Affairs. As she was new to her position (joined SF DPH last month) and substitute presenter, Katy read through her presentation and offered to follow-up “later” on questions. After she read "CDPH Allocation Strategy" slide listing SNF but no mention of other residential LTC facilities in Phase 1a, I asked about inclusion of other residential LTC facilities like assisted living? Katy said SF based on California DPH guidelines. If so, I noted (in Zoom chat) it would be helpful for SF DPH to be consistent with state DPH, which provided this language in Phase 1a: “Residents of skilled nursing facilities, assisted living facilities, and similar long-term care settings for older or medically vulnerable individuals.” “Later” SF DPH revised to conform with state.
Vaccination in LTC facilities took longer due to informed consent issues from residents with cognitive impairment or locating their proxies, and some health workers declined vaccination.

Katy read Phase 1b-Tier 1 listing age 75+ and certain at-risk of exposure essential workers in education/childcare (as there’s pressure to open up schools, and teachers’ union concerned about safety), emergency services, food and agriculture; Phase 1b-Tier 2 listed age 65+, as supplies allow.
Then six days later…on Jan. 25, California Governor announced change to age-based eligibility system after vaccinating health care workers, LTC residents, teachers, emergency personnel, and those age 65+. This latest change made to speed up process as much easier to verify age than seeking documentation for essential workers and high-risk medical conditions. Needless to say, this latest change provoked outrage among people with high-risk medical conditions, which is focus of SDA’s latest advocacy campaign.

At Jan. 21 annual meeting of Hawaii Pacific Gerontological Society (HPGS), Hawaii Lt. Gov. Josh Green (who also works as ER doc) presented on Hawaii COVID-19 update: from Mar. 7, 2020 to Jan. 16, 2021, Hawaii had 2nd lowest infection rate in U.S. (after Vermont, which is rural and smaller) and lowest COVID-19 death rate in U.S. Statewide mask wearing is 86% according to Hawaii Department of Health survey for week of Jan. 17.
COVID-19 impacts on health, housing and unemployment were less positive: 15% increase in Medicaid beneficiaries, bringing total to 380,000 (1 in 4 statewide); doubled call volume to National Alliance on Mental Illness (NAMI) Hawaii; 46% increase in calls to Domestic Violence Action Center helpline; 60% increase in food insecurity (1 in 5 statewide); and 11,000 households behind in rent.
As of Jan. 20,
Hawaii administered 45% (70,095/154,150) of vaccines received. Vaccination
distribution rolled out in phases: Phase 1a (Dec. 2020-Jan. 2021) focus on
healthcare workers and LTC residents; Phase 1b (Dec. 2020-Mar. 2021) focus on
Hawaii residents age 75+ (est. 109,000) and frontline essential workers on-site
and close proximity to others (est. 50,000).
A week later, 500 Hawaii State Capitol lawmakers and staff received COVID-19 vaccines as frontline essential workers in Phase 1b of vaccination prioritization alongside kupuna age 75+! How dare they get vaccinated before my parents age 75+, who are scheduled for their first COVID vaccine shots tomorrow?!
Though older adults are prioritized, many faced barriers to access information about availability and scheduling vaccination appointments in overwhelmed system with website crashes (plus digital divide with only 59% of older adults have home broadband services, exacerbated in low-income communities), lacking social supports and private transportation for long distances (especially in rural areas) and/or drive-through vaccination sites, waiting in long lines without access to toilets, and prospect of repeating process for 2nd shots!
Whites are getting vaccinated at higher rates than members of historically
marginalized groups who may not live to eligibility age 75 or 65 (Black men, LGBT,
unhoused, etc.), which raises issues of equitable access, particularly under California's latest age-based system.
Equity efforts focused on COVID-19 racial/ethnic disparities. SF Human Rights Commission hosted two-part series exploring the racial history of pandemics to inform equitable access to vaccination and recovery, with representatives of impacted communities to address vaccine hesitancy and engage access (language and culture). Part 1 Pandemic within Pandemics: The Racist History of Disease looked at the past to help understand the present and prepare for the future, because to ignore history is to repeat it. Waves of disease (cholera, 1918 Influenza, HIV/AIDS, COVID-19) often trigger a social pandemic of hatred, racism and xenophobia, while exacting its heaviest toll on traditionally vulnerable communities. Almost one year into COVID-19 pandemic, BIPOC communities bear the brunt of the pandemic.
The program featured community leaders starting with Indigenous Elder Mary Travis Allen, who opened with land acknowledgement, and American Indian Cultural Center Executive Director April McGill shared history and generational trauma of indigenous people decimated by infectious diseases brought by white colonists/settlors, who exacerbated mistrust by infecting blankets with smallpox.

Valerie Tulier-Laiwa, Coordinator of Latino Task Force for COVID-19, discussed politics and epidemics (scapegoating migrants as disease-carriers); eugenics and unethical clinical trials (Puerto Rican women used as guinea pigs for Enovid birth control pills); California targeted Latinas for forced sterilization; allegations of “mass hysterectomies at ICE.” She concluded with take-aways to engage in community with the first wave of vaccinations, empower and listen to those doubly impacted by stigma and disease.

Patsy Tito, Executive Director of Samoan Community Development Center (SCDC), shared challenges faced by Pacific Islanders who make up less than 1% of SF population, small so less visible and harder to draw attention to needs, sometimes categorized with Asians; yet, PIs have highest per capita cases of health disparities; many do not have healthcare because some undocumented or lack access to resources—took her 6 months to get COVID test; heartbreaking to be separated from family, especially elders; silence no longer an option. (Awesome to hear from Patsy, who I met years ago when she advocated SF Department of Aging & Adult Services to replace western meals with more culturally appropriate Polynesian foods for SCDC’s Senior Center to boost participation. SCDC became model for American Samoa’s own senior congregate lunch program!)
Ayanna Bennett, MD, SF DPH Director of Health Equity, discussed how history of medical experimentation, racial discrimination in health care systems, implicit bias in medical decision-making, etc. make it difficult for BIPOC to seek out and receive appropriate care. She asked that we reframe vaccine hesitancy as an assumption of logical choice based on awareness of history (e.g., 1932-1972 Tuskegee syphilis deception using Blacks for data collection v. treatment; segregated care/denial of treatment access for Blacks during 1918 flu pandemic and polio epidemic until 1950s vaccine; 1981 HIV disproportionate impact on Blacks until 20 years later dedicated federal program specific to Blacks). Dr. Bennett advised to challenge system by asking these questions to prove whether trustworthy: Equal information? Equal risk? Equal access? Equal options?

Part 2: Understanding Community Response to Vaccines: An Anti-Racist Approach featured Michael Liao, NICOS Chinese Health Coalition Programs Director, presented on Building Trust with Chinese Community, discussing importance of:
·
understanding
client’s language, dialect, and literacy levels; non-verbal
language/communication, such as saving face & deference to authority;
differences in communication patterns (eye contact, emotional expression)
·
Recommendations:
don’t assume smiles & nods mean client agrees/understands you; ensure
comprehension, ask clients to repeat info back to you; exhibit empathy by
mirroring gesture & tone
·
understanding
client’s socio-political experience that may have clinical implications, pre-
& post-migration (e.g., persecution by one’s own government back home), and
discrimination/exploitation (e.g., being targeted by scammers disguised as
authority figures)

When Michael discussed working with the family, not just the individual, I thought this is actually very common when working with older adults – either by client consent or family member is power of attorney/proxy. Also important to consider client’s level of assimilation/acculturation by asking about client’s expectations.
Michael shared organizational strategies, such as ensuring that service providers look like those they are serving, speak like them and are sensitive to their needs; diverse representation in agency workforce at all levels; bilingual and staff of color are supported; training on cultural humility and competency. (NICOS provided resource list of language interpretation and translation services.)

Dr. Bennett said SF vaccine rollout's chief obstacle is not enough doses, while SF DPH continues to partner with hospital systems to quickly and efficiently get people vaccinated; ensure those most impacted by virus have access to vaccine; commit to ensuring transparent and easy process; follow 3-pronged distribution strategy to high-volume vaccination sites, community-based distribution (mobile, hubs, clinics), and pharmacies.
Safety
net
Government budget deficits are unraveling the old-age safety net, leaving seniors on waitlist for in-home aides and home-delivered meals.
Gray
Panthers hosted Zoom meeting to discuss SF budget crisis and its impact on services
to seniors and adults with disabilities.
Due to loss of revenues and continued uncertainties about recovery from
COVID-19 pandemic, SF Mayor requested that all City departments reduce General
Fund budgets by 7.5% in each of the next two fiscal years; priorities to support
City’s economic recovery, COVID response, homelessness services, and
initiatives that advance racial equity.

Marie Jobling, Executive Director of Community Living Campaign and Co-Chair of SF Dignity Fund Coalition, explained due to hard economic times, Dignity Fund will not receive annual allocation of $3 million for next two years. Marie noted housing continues to be the biggest driver of living costs for SF residents, who require $4K per month to live alone, according to Elder Economic Security Index; she leaves housing advocacy to SDA. Her advocacy focus will be on changing Medi-Cal asset limits (currently $2K for single, $3K for couple, unchanged since 1989).

Shireen McSpadden, Executive Director of SF Department of Disability and Aging Services (DAS), explained that federal CARES Act funds offset some local funding in Elder Justice and food assistance. IHSS 7% cut in hours have been restored; hourly wage increases, which were suspended due to economic downturn, will be implemented to $17.50 on Feb. 1, 2021, $18 on July 1, 2021, and $18.75 on July 1, 2022. She concluded with need to remain vigilant—e.g., state’s early COVID crisis guidelines discriminated against older age until advocates fought back—because it’s “hard to get people to care about older adults and people with disabilities.”
Gray Panthers support a wealth tax on American billionaires who benefited from tax cuts and deregulation under Trump.

Kevin Prindiville, JD, Executive Director of Justice in Aging (JIA), delivered keynote at Senior Services Coalition (SSC) of Alameda County’s Making the Difference Together: Taking Stock of the Aging Policy Landscape in 2021 conference via Zoom.
Kevin
said coming up in March, JIA will announce its new strategic initiative to
advance equity in aging, ensuring all its programs—trainings, policies, class
action litigation—are centered in equity, in particular racial equity. He
described JIA’s internal work for the past five years to build a more inclusive
and equitable culture, starting with a need for more diverse staff, and
bringing in consultants to build a more inclusive culture to enable everyone to
do their best work. He acknowledged this
internal work involved willingness to be uncomfortable and vulnerable around
identity, confronting one’s own privilege (fragility?), but trust in the intent
with the idea of moving forward and growing, as diversity enabled more
considerations to inform decision-making and more power to connect with more
diverse partners with lived experiences to find better policy solutions. In this process, they were in a better
position to understand the “massive inequities that face people as they age” and
the cumulative impact of systemic structural inequities like racism, sexism,
homophobia, ableism, nativism, etc. as people grow older that lead to huge
disparities in poverty, economic security and access to health care. These
disparities are more pronounced based on race, among BIPOC.
Kevin
noted that JIA has been focused on fighting poverty for almost 50 years, but
realized “fighting poverty is not the same as advancing equity.” At the same time, he says they “get pushback
from the aging community about talking about (racial) equity too much” and
resistance from other communities who don’t see age as an equity consideration
when California decided to prioritize vaccination for people 65+, instead of
equity considerations for essential workers, younger people with chronic health
conditions, etc.
To address the diversity in pipeline issue, given the lower numbers of BIPOC law school graduates, Kevin decided that their hire for newly created Director of Equity & Racial Justice Advocacy would not need to be a lawyer.
(Pandemic
has accelerated equity by doing away with standardized testing in many college
admissions; historically merit-based selective Lowell High School in SF will be
under lottery system for upcoming academic year, and possibly indefinitely to
diversify student body.)

After Kevin’s keynote, my next favorite part of this conference was listening to advocates describe Prizes to Keep Our Eyes On: Wendy Peterson, Director of SSC, wanted to expand Adult Protective Services’ Home Safe (homeless assistance and prevention) program beyond sunset date of June 2021, and promote digital inclusion for seniors and low-income communities by expanding broadband connectivity to affordable/subsidized housing.

My prize idea: More organic cotton shirts, union printed with image of Bernie’s sensible chic to raise $ for aging services, like nearly $2 million within five days for Meals on Wheels and other charities!
SF public school teacher called out Bernie’s fashion at inauguration as white privilege, but didn’t call out Janet Yellen who was dressed similarly. Seems more like old people privilege in operation as 79-year-old Bernie and 74-year-old Janet were dressed appropriately in waterproof parkas in windy and snow flurry day because older people can lose body heat fast.
“Bernie wore something that is accessible to normal people. People can't afford those lovely outfits that everybody else wore, although they were nice to look at. It was nice to have a little piece of reality, you know, and of normal people in such a prominent event.”—Jen Ellis, “Meet Jen Ellis, The Woman Behind Bernie Sanders' Inauguration Day Mittens,” NPR (Jan. 21, 2021)

https://www.fa-mag.com/news/how-stocks-did-under-president-trump-59887.html
I
confess: When I hear “equity,” I think ownership interest in an asset such as equity
security (stock), or investment of financial capital. After all, much of my career was focused on
equity investing in retirement portfolios, and the language is similar (plus good
stuff for working stiffs to know!): the value of equity in asset allocation
based on time horizon and risk tolerance, with diversification
across different asset classes, companies, industries, and geographies. As people get closer to accessing retirement
funds, increasing exposure to bonds/cash helps to buffer decline in more
volatile equity (risk-reward). This was
mostly color-blind, except for “green” investing. Similar to affirmative action,
tax laws governing qualified retirement plans enable a form of wealth distribution:
during annual compliance testing, a tax-qualified plan that is deemed to disproportionately
benefit/discriminate in favor of key employees (company owners/officers)/highly
compensated employees requires the plan sponsor (employer) to make contributions
to non-key/non-highly compensated employees. Outside of qualified plans, investment
in equities has cumulative advantage of long-term capital gains taxed at
rates lower than ordinary income.
Now
equity is so racialized in USA, and this racial reckoning is long overdue. Yet equity is multi-dimensional, identities
are intersectional, and these considerations are more important as older adults
become more heterogeneous with age.
Older Americans Act, which provides federal funding of home and community-based programs for older adults, uses equity standards in targeting older adults with the greatest economic or social need and those who are at risk for institutional placement. Older Californians Act specifies low-income, non-English speaking, minority, and frail persons. SF DAS priority populations are persons who are socially isolated, with low-income, with limited English-speaking proficiency, from communities of color, who identify as LGBTQ, and at risk of institutionalization...so we can live equitably after all!

Wow! During walk in my neighborhood, spotted these abandoned gerontology books... hope someone picks up on them! I've kept my gero books for reference because aging is our present and future!