
At this month’s American Association for Geriatric Psychiatry (AAGP) virtual meeting of curious minds, AAGP President Brent Forester, MD, MSc, welcomed 1,205 attendees, noting 25% are trainees (222) and students (58). (At $20 member student registration rate, best investment ever!) Due to COVID-19 pandemic, last year’s annual meeting was canceled, and Dr. Forester said he was glad to be back attending his 25th AAGP meeting.
I was glad to attend my 2nd AAGP meeting—even if this was virtual and not in Hawaii (with fab food!) like my 1st AAGP meeting.
As expected, this
meeting offered many sessions on Alzheimer’s disease (AD) and related dementia,
cognitive decline, and depression. (These are related issues based on research
finding that older adults with recent mild cognitive impairment or
dementia diagnoses were at increased risk of attempting suicide.) On-demand sessions, which attendees can
access over next six months, offered more varied topics: forensics, moral
injury/stress first aid, hoarding disorder, productive aging and creativity, late
life schizophrenia, psychotic depression, geroscience and mental health, sex
differences in late-life neuropsychiatric disorders, etc.
Starting
after Daylight Savings Time, AAGP’s weeklong meeting provided virtual daily
program from 11 am to 4:30 pm EDT, with 15-30 minute breaks to rest our eyes
from screens.

Dr. Forester (talking head in clouds?!) shared why he got into geriatric psychiatry, and his reasons were similar to why I entered gerontology field: family role models (grandparents); advocacy efforts are critical; many research questions await investigation; holistic and comprehensive approach to dementia (neurobiological, clinical syndrome, family/caregiver, community, population); and interdisciplinary care team.

He discussed the impact of COVID-19 and geriatric psychiatry. Challenges: disparities based on age, race/ethnicity; long-term care (LTC) calamity; barriers to accessing technology; social isolation. Opportunities: telehealth effective (almost like house calls); renewed focus on geriatric mental health, financial and psychosocial impact of dementia; studying psychiatric medication to combat COVID-19.
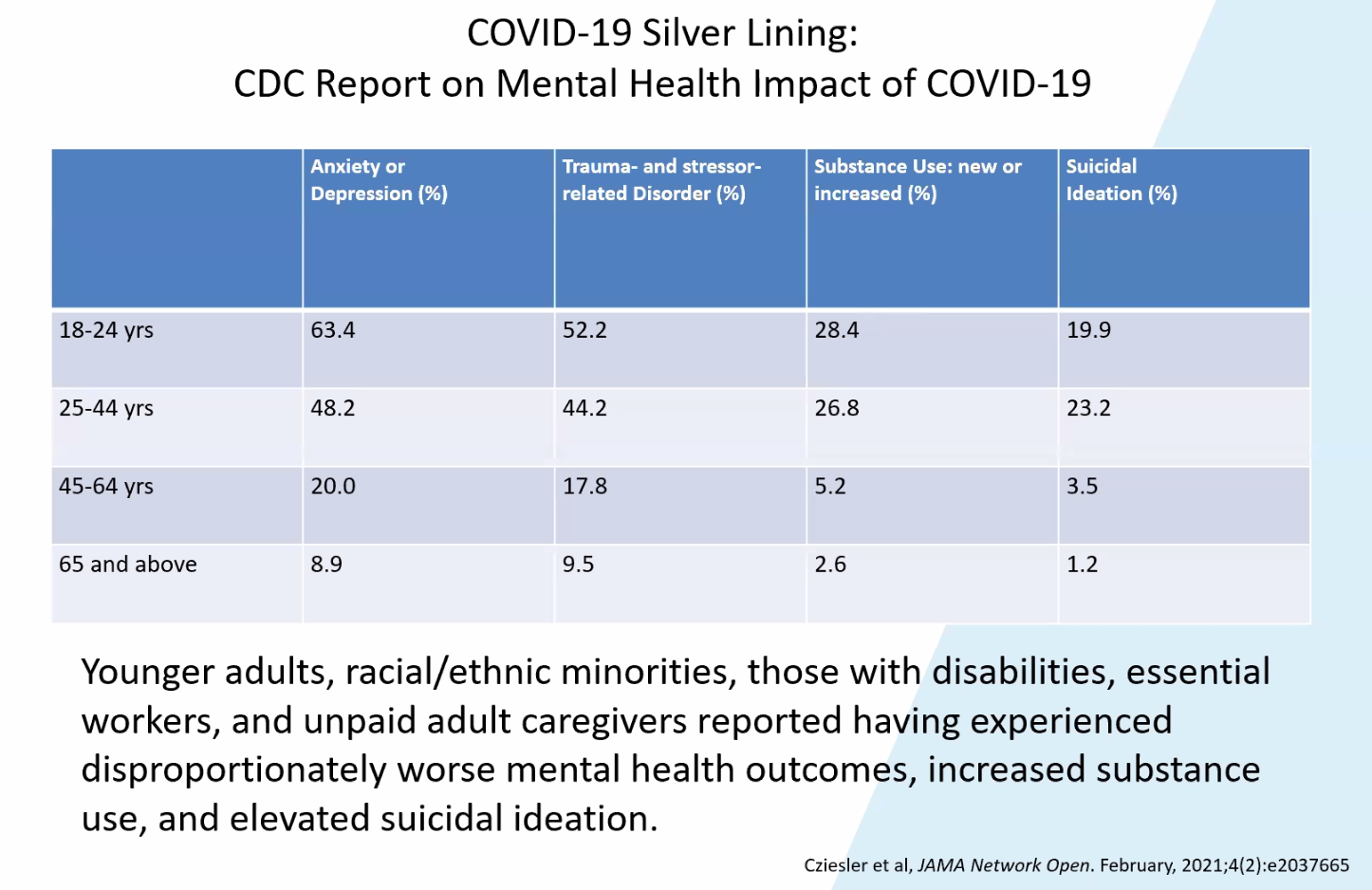
Despite their increased COVID-19 related morbidity and mortality, older adults age 65+ experienced less adverse mental health symptoms among age groups who completed internet-based COVID-19 Outbreak Public Evaluation (COPE) surveys in September 2020. Dr. Forester discussed how older adults age 65+ might be more resilient to adverse mental health outcomes than younger age groups during COVID-19: internal factors (cognitive capacity, personality, physical health); external factors (social status, financial stability); countering loneliness via “oneliness” (ability to be alone but content); wisdom (empathy & compassion; emotional regulation; ability to self-reflect; acceptance of diverse perspectives; better social decision-making; spirituality).
[External factors like social determinants of health impact one’s resilience and measure of well-being/happiness. A survey, conducted last month by the Harris Poll, found that many parents of children under age 18, essential workers, younger people and Black and Hispanic people have experienced disproportionate share of pandemic stress. Younger adults were most likely to admit their mental health worsened during this pandemic (less stigma might be a factor?). Findings from a study on age differences in psychological well-being during pandemic based on University of Michigan data: older people reported less pandemic-related stress, less life change as they were likely already retired and spend more time at home, less social isolation, and lower negative relationship quality than younger people. In contrast, younger people may be relatively more vulnerable to pandemic-related stress and social isolation due to greater life changes related to university closures, moving back home with parents, increased unemployment/reduced income, etc. Excessive screen time appears to be messing minds of young people attending Zoom school--so much that last month SF sued its own School District and Board of Education for failing to reopen schools for in-person instruction, while Board (facing recall) was distracted renaming 44 schools.]

Love this slide from Dr. Forester’s presentation, which highlights the value of empathic curiosity and listening to the lived experiences of people and their support network for a “comprehensive, longitudinal and interdisciplinary treatment plan”…and acknowledges how this essential work may be hampered by shortage of providers with expertise and motivation to serve older adults.

After discussing context of health care “transformation” (past v. 2021: care built around institution v. patient; payments incentivize more v. better care; responsible for immediate outcome v. ongoing health; grudging acceptance of cost v. unable to sustain cost burden), Dr. Forester highlighted role of geriatric mental health in “epicenter of population health strategies” to improve quality of care at individual and population levels, while reducing overall costs of care given behavioral health + geriatric care as drivers of health care spending (especially AD as “long-term epidemic of our time”). He discussed interdisciplinary models of dementia care: Mass General Brigham Memory Care Initiative; UCLA Alzheimer’s Dementia and Care Program; and CRESCENT (lower cost adaptation of UCSF Care Ecosystem).
During mid-day break, time to visit Exhibit Hall and Speed
Roundtable Topics!

Stopped by to see Meet AAGP Presidents, including Elliott Stein, MD (AAGP President 1985-87) with whom I had the pleasure of working during my stint at SF Campus for Jewish Living, where he was Medical Director of the Acute Geriatric Psychiatric Hospital and available for consultation during interdisciplinary team meetings involving long-term residents. This Zoom meeting is also closest I’ve gotten to Marc Agronin, MD, author of Therapy with Older Clients: Key Strategies for Success (2010)--my cherished go-to book, and love his explanation on why older people do not need bucket list! Current AAGP President Forester specializes in older adult bipolar disorder (OABD).

Next moved over to Perspectives from Senior Geriatric Psychiatrists with Dilip Jeste, MD, Director of University of California San Diego Center for Healthy Aging, known for his research on wisdom in later life and advocacy for multigenerational activities; and Helen Lavretsky, MD, UCLA geriatric integrative psychiatrist known for her research in complementary and alternative therapies for mood disorders.

Laura Gitlin,
PhD (sociologist), Dean of the College of Nursing and Health Professionals at Drexel
University, presented on Home and Community based Interventions for Dementia
Care: The Challenge of Bringing Evidence to Practice in pre-recorded video.
As viewers asked questions in chat
box, she responded in real-time. After video presentation, there was live
Q&A. She developed COPE (Care of
People with Dementia in their Environments)/TAP (Tailored Activity Program) as
non-pharma interventions intended to be built into routine care, including
integration with trained occupational therapists, nurses and recreational
therapists. Because the therapeutic relationship is critical, caregivers who
are clinically depressed may need their depression addressed first or simultaneously
with COPE/TAP. There are ongoing pilots
to support reimbursement potential for COPE/TAP through Medicare Part B.

William Reichman, MD, Baycrest (Toronto) President & CEO, presented on LTC Across the Globe. In Canada, over 80% of COVID-19 deaths occurred in LTC facilities so there is growing movement to reform industry and develop alternatives.
·
Pioneer Network advocates person-centered Culture Change Movement (1997) with innovations:
homelike environment; outdoor settings; choice in dining options &
scheduling of activities; ambient sounds, pleasant music; programming including
pets & children; staff have flexible roles & responsibilities;
residents & family engagement in healthcare planning
·
WHO defines LTC as service v. facility, an integrated
system—affordable & accessible by poor & marginalized; uphold human rights
of care-dependent older people; enhance older people’s intrinsic capacities;
person-centered, oriented around needs of older person; LTC workforce treated
fairly, with social status & recognition it deserves; national governments
take overall responsibility for stewardship of LTC systems—strategies to enable
aging in place that is equitable and sustainable.
·
Alternatives
to nursing home model include: “age-proof” Dutch Apartment for Life; Naturally Occurring Retirement
Community (NORC); Accessory Dwelling Unit (ADU); Dementia Village (Hogeweyk);
US Green House/Small House Model
[In “Nursing
homes need fixing. Here’s where to start,” Harvard Health Care Policy Professor
David C. Grabowski, PhD, recommended these ways to improve staffing for better care: increase minimum staffing levels of direct care workers; increase staff
pay and benefits; raise Medicaid reimbursement; increase financial transparency
(to ensure public dollars spent on staffing as policymakers intended); provide
career advancement; and create better work environment through culture change (by
empowering staff based on Green House model). Grabowski’s focus is nurse/nursing aides
staffing, yet I think staffing improvement should extend to social services to balance
medical model with psychosocial support to residents.]

Kristine Yaffe, MD, Director UCSF’s Center for Population Brain Health, presented Dementia Prevention at the Population Level: Modifiable Risk Factors. She noted following trends: dementia prevalence has been lower or stable in several countries—associated with public health strategies, decreased cardiovascular disease, improved education and economic well-being. However, epidemics of sedentary lifestyle, obesity, and diabetes could have opposite effects.

Sleep is important to clear amyloid (plaques outside neurons) and tau (tangles inside neurons), biomarkers of AD-type pathologic changes in the brain. In people with advanced dementia, sleep is disturbed, sundowning increased, nighttime sleep fragmented; poor sleep quality is associated with cognitive decline, and thus might be used as early marker for AD.
Lancet Commission on dementia recommended interventions for 12 risk factors, considering a life course perspective and tackling inequality: childhood education, exercise, social engagement, smoking, management of hypertension, hearing loss, depression, diabetes, obesity, excessive alcohol consumption, head injury, and air pollution.


During Dr.
Tariot’s discussion of pharma approaches, there were technical difficulties
including overlapping audio streams…amusing so chat box filled with comments
like “wow, live demonstration of DRP” and “welcome to the world of a patient
with DRP.” (At 2018 AAGP meeting, I participated in Parkinson’s Psychosis
Simulation wearing Oculus Virtual Reality headset, which projected
visual-auditory hallucinations that were mind-blowing!) In their summary (take-home points slide above), they
noted dementias are increasing in prevalence (contrary to Dr. Yaffe’s earlier
slide, but perhaps they are looking at different time periods?).

Self-examination was focus of Ageism: A New Look at an Age Old Problem. Susan W. Lehmann, MD, Johns Hopkins School of Medicine Professor (and co-author, with Dr. Forester, of Bipolar Disorder in Older Adult Patients), considered Dr. Jonathan Maltz’s When should an aging doctor call it quits? (published in WaPo, Mar. 31, 2019; at age 70, Dr. Maltz justified practicing medicine part-time because of his sharp mind, good health and hope that old age “has allowed me to acquire greater wisdom, compassion, resilience and stress tolerance”).
Should aging physicians (23% are age 65+) be subject to cognitive and psychomotor testing to continue practicing medicine, particularly surgeons whose skills depend on manual dexterity? Is this “fair” or age discrimination? Sir William Osler (1849-1919), co-founder of Johns Hopkins Hospital and considered Father of Modern Medicine, recommended retirement at age 60… at a time when life expectancy was much lower than today.
Dr. Lehmann
noted aspects of cognitive aging that can impact physician clinical performance:
crystallized intelligence better preserved than fluid intelligence; language
skills intact, especially vocabulary; memory changes (decreases in semantic,
working, and episodic memory); vulnerability to decreased processing speed (harder
to complete complex tasks), and declines in hearing/visual acuity.
While there is great variability in cognitive function, Dr. Lehmann noted some concerns about older physicians impacting patient care: older physicians found to have less factual knowledge, less adherence to standards of care, poorer patient outcomes; older surgeons less likely to incorporate new approaches into practice; and patients treated by older physicians had higher mortality than patients cared for by younger physicians. Further, physicians may not recognize their own impairment, as individuals with neurocognitive disorders often minimize/deny impairment, or lack insight/awareness of deficits; ageism/stigma may prevent them from seeking help; and counting on colleagues to refer physician whose performance adversely affected by cognitive/physical changes is not reliable.
American Medical Association (AMA) and Society of Surgical Chairs (SSC) considered, but never adopted, age-based screening/assessment for physicians, because this might worsen existing physician shortage; however, hospitals monitor and review age-based practitioner screening programs for mental and physical acuity.

Mary Blazek, MD, of Michigan Medicine (and English Lit major!), explored Combatting negative attitudes toward older patients in medical students: Are Arts the answer? She found that students enter medical school with ageist attitudes, which likely worsen over time and influenced by attitudes of senior physicians and “hidden curriculum”; and interventions to improve attitudes yielded mixed results. These interventions included making ageism explicit; open discussion/self-reflection; small group learning; patient-centered curricula; better integration of marginalized groups; humanities education. She expressed concern that in virtual learning during this pandemic, students miss “joy” and “liveliness” of in-person interactions, and thus may not be attracting students into geriatrics field.
Dr. Blazek’s presentation suggested that arts promote empathic curiosity, which was reinforced in Association of American Medical Colleges’ report, The Fundamental Role of Arts and Humanities in Medical Education (Dec. 2020).
According to Dr.
Faith T. Fitzgerald, geriatrician and former dean of students at University of
California at Davis School of Medicine, curiosity is the most important
characteristic for medical students being viewed as more humane; key was taking a lot of courses, and
it didn’t matter whether they took humanities or science courses. She explained:
“What is kindness, as perceived by patients? Perhaps it is curiosity: ‘How are you? Who are you? How can I help you? Tell me more. Isn’t that interesting?’ And patients say, ‘He asked me a lot of questions’; ‘She really seemed to care about what was going on with me.’”—Faith T. Fitzgerald, MD, “On Being a Doctor: Curiosity," Annals of Internal Medicine (1999)
In a nutshell,
the field of geriatrics/gerontology needs more curious people or lifelong
learners to combat ageism!

Piruz Huda, NP, presented Integrating Non-pharmacological and Pharmacological Interventions in the Treatment of Behavioral and Psychological Symptoms of Dementia (BPSD), based on his contributions to Staff Training in Assisted Living Residencies (STAR) for dementia care. STAR has been adapted for family caregivers (STAR-C) and VA Community Living Centers (STAR-VA).
(Recent study from University of Toronto found non-drug therapies to be as good or better than medications in treating depression in patients with dementia.)

In Equity, Racism and Healthcare Delivery Systems: COVID and Beyond, Thomas Sequist, MD, MPH, Chief Patient Experience and Equity Officer at Mass General Brigham Healthcare System, provided an overview of racial and ethnic health disparities related to COVID-19; described systems- and community-based intervention strategies to promote equity and advance anti-racism in healthcare, both during the COVID-19 pandemic and beyond. His approach to addressing equity was similar to safety process: resource it (training, counseling, policies), hold accountable and elevate to stated goal. Hospitals are used as a gap in the social safety net, and cannot solve all structural racism.
Interesting to hear medical profession’s acknowledgement of racism after last month’s controversial JAMA podcast and tweet questioning existence of structural racism in medicine. See NPR’s “'Providers Don't Even Listen': Barriers To Alzheimer's Care When You're Not White” (Mar. 2, 2021). In Jan. 2021, American Psychiatric Association (APA) issued apology to BIPOC for structural racism in psychiatry, after APA President Jeffrey Geller, MD, MPH, formed Task Force to Address Structural Racism Throughout Psychiatry and published 9-part series on Structural Racism in American Psychiatry and APA last year.
Last week, UCSF launched Racism and Race: The Use of Race in Medicine and Implications for Health Equity Event Series.
This AAGP
meeting of minds reminded me of the value of diversity and inclusion (theme of
2018 AAGP annual meeting) in person-centered care, as the ultimate
question is what does the individual want…to be called? how to be treated in this
life on earth? to die alone? So important to advocate for equity to meet people
where they are, and offer culturally and linguistically relevant support
services.
Ageism

By coincidence, as AAGP held its ageism session on Mar. 18, United Nations declared Ageism is a global challenge and issued a report with WHO calling for urgent action to combat ageism including better measurement and reporting to expose ageism with harm to older and younger people who have been stereotyped in public discourse. During COVID-19 pandemic, age has been used as the sole criterion for access to medical care, lifesaving therapies and for physical isolation.
Media have a role in combatting ageism, and older people are more visible in this year’s Oscar nominated Best Picture films (and Asians recognized as Best Director nominees): 83-year-old Best Actor nominee Anthony Hopkins portraying man experiencing dementia in The Father; 73-year-old Best Supporting Actress nominee Youn Yuh-Jung as caring grandmother in Minari (Lee Isaac Chung, also nominated for Best Original Screenplay); and 63-year-old Best Actress nominee Frances McDormand as van dweller in Nomadland (Chloe Zhao)! Also, interesting to see The Mole Agent, nominated for Best Documentary featuring octogenarian Sergio Chamy as undercover agent in a Chilean nursing home (unlikely to happen in USA)!
AARP released Age Diversity and Inclusion Worksheet for employers!

Joined SF Supervisor Gordon Mar’s District 4 Virtual Town Hall: Supporting Seniors, as an opportunity to ask about SF’s efforts to end ageism, but my submitted questions were ignored:
·
What’s the impact of SF Reframing Aging/End Ageism
SF campaign that was launched in Fall 2019?
Btw, I note this program is called Supporting Seniors, though Reframing
Style sheet refers to research to support changing language to change the
culture: use older people/older adults, which is perceived as “more capable”
than seniors. I know
many people age 60+ who prefer to be called senior as more honorific term.
·
As SF reopens, are there plans for more intergenerational
opportunities as age segregation appears to “other” seniors/older people?
Attendee Esfir commented in chat box: “Older adults could be any
age, 20 years old is older adult for a child. We are seniors, we can be
recognized right away, otherwise there will be a lot of confusions.” My response: “Agree, people should be called
what they want. Thank you!”
Anyway, panelists talked about pivoting in-person to virtual services during pandemic, including food (March is Senior Nutrition Month!) which was made available for pick-up (no congregate dining) or delivered to seniors at home.
· Self-Help for the Elderly CEO Anni Chung spoke about her agency’s efforts to vaccinate clients
·
SF Department of Disability & Aging Services (DAS) Executive Director Shireen McSpadden discussed plans for mobile units to
vaccinate homebound seniors
·
Community
Living Campaign Connector Margaret Graf announced that her in-person Senior
Power meeting reopens next month, in an open-air tent as drop-in senior center,
with activities like watercolor painting and poetry reading—while observing
masking and physical distancing.
My question about intergenerational
opportunities was partly answered when I received agenda for next week’s DAS
Commission meeting that will consider granting $1.3 million to senior centers
for intergenerational programming. Ok, and why not make more organic intergenerational
connections at integrated spaces at lower cost?
“We need to be creative in bringing older and younger people together through daily encounters and the discovery of shared interest — through proximity and purpose. Down deep, there's self-interest running up and down the generational chain. We need each other.”—Marc Freedman, “My COVID-19 Experiment With Multigenerational Living: Could I survive a dose of my own rhetoric when my in-laws moved in behind our house?” Next Avenue (Mar. 24, 2021)
More violent
elder abuse

While COVID-19 hospitalizations and deaths of older people have decreased (thanks to vaccine), reports of elder abuse have increased at frightening pace… often caught on surveillance video, followed by GoFundMe campaigns for victims, and more mainstream media coverage of Asian victims (mostly monolingual, non-English speaking immigrants) by SF Bay Area ABC7 anchor/reporter Dion Lim (herself a daughter of Chinese immigrants) as she has interviewed older Asian victims like 84-year-old Rong Xin Liao who was waiting for bus when 23-year-old male kicked him off his seated walker causing his head to hit the ground in SF Tenderloin.
· 26-year-old male suspect robbed and knocked to the ground 75-year-old Pak Ho (Chinese), who had been taking his usual morning walk in Oakland Chinatown and died two days later
· 39-year-old man attacked 83-year-old Ngoc Pham (Vietnamese), and then 75-year-old Xiao Zhen Xie (Chinese), in SF Downtown near Civic Center Farmers Market; unknown whether attacks were racially motivated hate crimes, but Ms. Xie, who fought back attacker after he punched her face, decided that $1 million donated to GoFundMe for her medical expenses would be donated to Asian American community to combat racism
· Three 19-year-old men arrested in attack and robbery of 67-year-old Asian man inside SF Nob Hill/Chinatown laundromat
· Three females (16-year-old suspect arrested) attacked 75-year-old white woman, robbing her purse and keys in carjacking in Safeway parking lot in SF Richmond District
· 32-year-old man fatally stabbed 67-year-old Carol Brown (his mother on Zoom call) and 69-year-old Kenneth Preston (his uncle) in their Altadena home
· 38-year-old man (on parole for killing his own mother) kicked to the ground, yelled “you don’t belong here” and then repeatedly kicked head of 65-year-old Vilma Kari (Filipina), who had been walking to church in New York
With so much anger and violence in the community, more important to connect older adults to Aging Services network because service providers are mandated reporters of suspected elder abuse—even when older adult is reluctant to report to law enforcement. Increased social support for older adults may prevent them from becoming victims of elder abuse, and protect them from negative outcomes of abuse (depression, anxiety).
“Why is the world finally paying attention to crimes against Asians? Because so many vulnerable senior citizens are being attacked…the people who should be respected and honored, which is at the very core of Confucianism.” –May Lee (Mills alum), May Lee Show #55 Respecting Our Elders (Feb. 18, 2021)

Masks protect against coronavirus,…but what does it mean to say “community protects its own” when the most common racial perpetrator for any victim is the same as the victim—except “when victims were Asian, there were no statistically significant differences between the percentage of incidents in which the offender was perceived as Asian (24%), white (24%), or black (27%)”--according to U.S. Department of Justice (DOJ) reporting of Table 14, Percent of violent incidents, by victimand offender race or ethnicity, 2018). (Why did DOJ’s Criminal Victimization report, 2019, exclude reporting Asians as victims in Table 16?!)
Speaking about anti-Asian racism seemed to be silenced out of fear that this might “take away from anti-Blackness”…until Mar. 16 mass shootings killing six Asian immigrant women (three were age 60+: Soon Chung Park, 74, Suncha Kim, 69, and Yong Ae Yue, 63) in massage parlors, which the 21-year-old white male shooter with sex addiction mansplained that he wanted to “eliminate” source of his “temptation.” Suddenly, blaming white supremacy became common cause for outpouring of solidarity with Asians, formerly invisible until viral videos of anti-Asian attacks…and re-examination of massage parlors as fronts for prostitution/human trafficking.
Given generational divide over how to respond to attacks on older Asians (mostly immigrants who want more police for protection v. younger, mostly American-born who seek community solutions like investment in mental health), SF Mayor Breed decided to please both: day after Atlanta mass shootings, she immediately directed police to increase patrols in “areas with high number of Asians” and then week later, she announced plans for Community Safety Teams and Senior Escort Program. Also, SF Police Department established a Community Engagement Division to address racist incidents, including an anonymous tip line for Cantonese and Mandarin speakers.
Asian and Pacific Islander Older Adults
Last Friday,
Mayor Breed announced plan to bring mobile vaccinations to Chinatown seniors. Finally, it has taken
a pandemic and rampant violence inflicted on Asian seniors for SF government to pay
attention to anti-Asian racism and marginalized Chinatown seniors who may
struggle with access to online systems and English only platforms for
vaccination appointments, as well as limited public transportation options and
safety concerns in getting to/from vaccination sites. And vaccination needs to be available to
others who live in close quarters with seniors, especially in single-room
occupancy hotels.

California Department of Aging hosted Culturally Informed Policy and Programs With and For Asian and Pacific Islander (API) Older Adults with two Asian presenters (Korean male, Taiwanese female) who barely mentioned Pacific Islanders and not much on Southeast Asian Americans.

Joon Bang, President & CEO of National Asian Pacific Center on Aging (NAPCA), provided overview of Asian American Pacific Islander (AAPI):
·
AAPIs age 55+ make up 4% of U.S. older
adult population, and 20% of AAPI population
·
AAPI is umbrella for 50+ unique
cultural identities & 100+ spoken languages. Because 56% of Asian older adults have
limited English proficiency (especially Hmong, Cambodian, Laotian, Vietnamese,
Korean and Chinese), language barriers can lead to isolation, loss of
opportunities, and prevent access to medical and social services
·
Historically, AAPI cultures are
group-oriented with emphasis on family as source of identity, traditional
household is multi-generational; filial piety (respect and care for older parents)
expected so AAPI families less likely to put older family members into
facility; 42% of AAPIs care for older adults v. 22% of general population.
Joon discussed “cultural competence best practices”;
however, because AAPI is not a monolith, cultural humility might make more
sense to recognize diversity: avoid assumptions, be curious and learn from
clients. And there is great need for
more culturally relevant home- and community-based programs—notably, On Lok’s
Program of All-Inclusive Care for Elderly (PACE) that has become a national
model.

Yvonne Sun, LCSW, Division Director of Special Service for Groups SILVER (Los Angeles), discussed some challenges in service delivery to AAPIs:
·
culturally
specific help seeking behaviors often are interpreted as “evasiveness” or
“resistance” to care due to indirect communication styles; collective
orientation involving family/community leaders as gatekeepers prior to
accepting care (may conflict with individual privacy in medical model); stigma
(concern with reflection on family system); trauma/immigration history with
public system/U.S. government (e.g., lack of trust by Filipino WWII veterans
who were promised but not given benefits); reliance on family caregiver
(expectation to take care of own)
·
language
proficiency
·
lack
of culturally appropriate providers/services
·
level
of understanding of service provider role
·
assessment
of need on incomplete/inaccurate data, thus lack of utilization of services
does not reflect lack of need in API community
·
avoidance
of confrontation in communication style might lead to dropping out of care (v.
challenging professional).
Yvonne’s best
practices included culturally appropriate delivery, which may include
collaborative style, taking time to build trust and allowing client to be
teacher, tailoring treatment to client’s interpretation of problem, being open
to non-traditional approaches, etc.
Justice in Aging selected attorney Denny Chan as its new Equity Advocacy Director, and posted video of him sharing how his work has been informed by historical inequities played out in his own family, including his 87-year-old immigrant Chinese grandmother who faced barriers accessing health care and services due to being limited English proficient and less physically mobile.
“Other” & belonging (via advocacy/engagement)

“Other” represents race/ethnic group with highest COVID-19 case rate in SF: 3.4% of confirmed cases yet only 0.5% of SF population!

According to SF Department of Public Health COVID-19 data tracker to date: 463 deaths (58.7% male; 61% age 80+, 17% age 70-79, 13% age 60-69, or 91% of deaths age 60+; 38% Asian, 21.4% Latinx, 27.6% White, 7.6% Black; 0.9% homeless). Total COVID-19 deaths: over 550K in U.S., over 2.77 million worldwide.
Last year COVID-19 displaced suicide as top 3 cause of death after heart disease and cancer, in U.S.
Tomorrow COVID-19 vaccine eligibility opens for age 50+, though very limited vaccine supplies; on April 15, vaccine eligibility expands to age 16+. Thrilled my turn for vaccination coming soon!!!
California ranks among the worst in U.S. for vaccine equity, so Governor Newsom (still facing recall efforts) wants to flood poor areas with vaccine.

California
Alliance for Retired Americans (CARA) hosted Fabulous Friday Forum with Josh
Kornbluth’s Citizen Brain monologue about his learning journey as Atlantic
Fellow for Equity in Brain Health at UCSF Global Brain Health Institute, followed by discussion with UCSF Memory
& Aging Center neuropsychologist Kate Rankin, PhD. During his fellowship, Josh realized that brain
health is a social justice issue, as he learned how inequality, poverty,
malnutrition, limited education, etc. among populations stunted brain
development.
Kate emphasized
that empathy does not mean agreement or forgiveness, but it is a “superpower of attention”
that calls on us to include everybody (their experience, their voice, their
truth) and ask what they want. One way
to build empathy is to hear each other’s stories of what brought them to where
they are, to understand more of the reality of the world we live
in through the eyes of the other person, by opening our minds and hearts to
stories that we weren’t expecting to hear, and keep listening. The process of incorporating other people’s
views then changes our brains, and empathetic people also have social
motivation (desire to help) to assert ourselves, like fight back if racists are
killing people of color!
This
empathy/attention sounds similar to cultivating “beginner’s mind” characterized
by curiosity, openness, and humility. Good points because political correctness/cancel
culture (so dominant in SF bubble)—being told what to think—is
antithetical to empathy, which involves how to think with greater
openness to other perspectives (and no need to agree/forgive).

In his latest video “Othering & Belonging” (Feb. 4, 2021) from Citizen Brain series, Josh offered democracy as solution so everyone belongs, favoring our kind/caring side over our primitive scared/angry side—urging “old folks to catch up”! Also, like the way he defines his multiple identities without reference to race and age because I find greater common ground and potential for engaging in more meaningful ways through Josh’s identities of being movie lover, museum goer, wearer of aloha shirts, etc.
“Democracy
had become the shared civic religion of a people who otherwise had little in
common… groups excluded from democratic government turned to democratic
governance to practice and press for equal citizenship…
This
is where the truly hard work begins.
Democratic governance is never the most efficient means of running an
organization, as anyone who’s attended a local zoning hearing can attest. Its value lies instead in harmonizing
discordant interests and empowering constituents. A nation of passive observers watching others
make decisions is a nation that will succumb to anger and resentment—witness
the United States.”—Yoni Appelbaum, “Losing the Democratic Habit,” The
Atlantic (Oct. 2018)
In new book, How Rights Went Wrong: Why Our Obsession with Rights Is Tearing America Apart (2021), Columbia Law Professor Jamal Greene criticizes how courts have framed rights as binary, all-or-nothing conflicts, with clear winners and losers; instead of discriminating between rights that perpetuate divisiveness, he proposes to reconcile competing rights with justice for all (i.e., weighing benefits/burdens of government action v. deciding values)!
“We have democratic institutions — legislatures and governors and mayors — precisely to reconcile our rights, through law. But first, we need to see each other as rights bearers and as equal citizens who disagree with one another but who must figure out a way to live together.”—Jamal Greene, “Americans are obsessed with ‘rights.’ In the pandemic, that’s killing us.” Los Angeles Times (July 2, 2020)
Transit is important to further mobility and connections to community, and pedestrians and drivers of motor vehicles need to figure out a way to travel safely. At SDA Transit Justice meeting, Walk SF organizer Brian Haagsman presented Vision Zero approach to “end all severe and fatal traffic crashes by 2024” because traffic deaths are preventable using a systems approach:
· prioritize safe streets first using data where most crashes occur to target improvements (high-injury network where top primary collision factors are drivers’ failure to yield to pedestrians, unsafe speed and not stopping at a red signal)
·
end
inequities in traffic violence, as low-income, immigrants, communities of
color, seniors and people with disabilities are twice as likely to live on
high-injury corridors
· address deadly speeds via automated speed camera enforcement, which has been reintroduced (AB 550) by Assemblymember David Chiu, with stronger protections for privacy and equity.
Assemblymember Phil Ting introduced AB 1283 (aka Freedom to Walk Act) to decriminalize jaywalking outside of a marked or unmarked crosswalk or against a traffic light when it doesn’t lead to an “immediate hazard”—in response to concerns of disproportionate enforcement against communities of color and need to prioritize enforcement against drivers. To date this year, four pedestrian deaths in SF included two seniors age 85 and 79, both in high injury corridors.

Gray Panthers hosted meeting focused on Long-Term Supports and Services for All! Michael Lyon reviewed Gray Panthers’ 6- Point Plan.

Lindsay Imai-Hong, California Director of Hand in Hand Domestic Employers Network, presented on Long-Term Supports and Services 4 All Coalition. Check out Quality Jobs Are Essential:California’s Direct Care Workforce and the Master Plan for Aging.

FrameWorks Institute
hosted Moving Mindsets-The Ways Minds Can Shift with Felicia Wong, CEO at Roosevelt
Institute, who talked about replacing the dominant neoliberal mindset with something
new and different “that is as yet unnamed.”
She noted that President Biden, as a moderate, traditionalist, creature
of the Senate, just signed $1.9 trillion COVID-19 stimulus package and promised
another $3 trillion to transform the economy including making care central—not
at all expected from centrist Biden a year ago—which could represent a mindset shift,
something deeper than a response to the pandemic to a culture of care that has
been missing yet necessary to move forward.
With FDR as his role model, Biden appears to be using Keynesian economics or deficit spending as an investment in our collective future. At age 78, Biden is much older than FDR (who assumed Presidency at age 51, and served for 12 years until his death at age 63) and has the advantage of “age-acquired wisdom to express a longer view of history.” Biden’s American Jobs Plan proposes $400 billion to expand infrastructure of care economy: “access to quality, affordable home- or community-based care for aging relatives and people with disabilities”!
This culture
of care resonates in Biden’s call for civility and riddance to bullying antics.
"If
you're ever working with me and I hear you treat another colleague with
disrespect, talk down to someone, I promise I will fire you on the spot…
Everybody, everybody is entitled to be treated with decency and
dignity."—President Joe Biden, Swearing-in his appointees (Jan. 20, 2021) https://thehill.com/homenews/administration/535142-biden-swears-in-senior-staff-and-warns-disrespect-each-other-and

Barbara shared her experiences as nurse, inspired to write her “little blue book” one year after Medicare hospice benefit began in 1984, explaining the “normal/natural” process of dying as a dying patient’s daughter took notes; afterwards, Barbara got out a legal pad and began writing like she was talking to someone who wanted to understand about how people die without being pathological, explaining that caring for people at EOL is different than getting better. At EOL, dying people might seek medical aid in dying (MAID).
“Seniors in the long-term care centres should be the ones who are speaking up and running the place. Some of them are not competent, that’s true. But many of them are. And they could take on the challenge.”-- 98-year-old Canadian retired geriatrician Ronald Bayne chose death at home by MAID over going into LTC facility, “Why did a geriatrician who fought to give seniors hope seek medically assisted death in the middle of a pandemic? He told us,” The Globe and Mail (Mar. 1, 2021)
According to palliative care physician Diane Meier, people request MAID for existential and spiritual reasons, and “the only treatment for that is relationship, attention, sitting with. Not trying to fix. That willingness to be with and engage the person in giving voice to that suffering.” But human connection is more distant during this pandemic.
Barbara took
issue with No One Dies Alone (NODA) when family/significant other of the
dying person wants it more for their comfort than the dying person who may not
care. Susan chimed in, recounting
experience of NODA being imposed on a reclusive person who seemed to wait to be
left alone to die.

During this Social Workers are Essential month, NASW-CA hosted Advance Directives 101 with Mario Espitia, LCSW, a palliative care social worker who said he learned on-the-job since most MSW programs do not address death and dying. Coming up Apr. 16: National Healthcare Decisions Day!
Better
dead than co-ed?

March is Women’s History Month, and Mills College Her-story looks like it might become history, another COVID-19 casualty? Mills grad student Paige inspired some hope, sharing her experience as an engineering undergrad at Sweet Briar when it faced closure due to financial challenges from both declining enrollment and endowment in 2015, but survived as a private women’s college due to alumnae’s legal actions and “Saving Sweet Briar” fundraising.
What
is happening with Mills College is not unprecedented. Women’s colleges have
suffered from declining enrollment in recent years, with several forced to
close or start admitting men in order to survive. There are just 34 women’s
colleges left in this country, down from 230 about 60 years ago…
This isn’t the first time the Mills community has gone up against challenge. Mills has survived the Civil War, World War I, the Depression, and World War II. In the 90s, student protesters occupied the campus for 13 days, rescinding school leadership’s attempt to start admitting men. The tenacity of the Mills community is boundless, organizing to Save Mills is happening, but is it enough?—Molly Curley O’Brien (Mills alum), “A Requiem For Mills College,” KQED (Mar. 24, 2021)
Mills
enrollment dropped sharply after 2014, following termination of experienced admissions
staff and elimination of Alumnae Admissions Representative program. [Huge
mistake because students see their future among alumnae in recruiting process—like
Hazel Soares (1915-2019), who graduated from Mills at age 94, proving
it’s never too late to use hubby’s GI benefits from WWII to pay for college!] Instead, former Mills President (corporate
attorney, with no academic teaching/publishing experience, who ultimately
resigned in 2016 while facing faculty no-confidence vote) relaxed admissions
standards by going test-optional (as done at Smith College since 2008) and
allowing non-binary/transgender applicants who self-identify as female.
On Mar. 17, Mills announced plan to cease as degree-granting college in 2023—171 years after its founding in 1852—and transition to a think-tank to promote women’s leadership and advance gender and racial equity. But not so fast, as an exciting intergenerational Save Mills College Coalition is fighting to preserve women’s college tradition for all ages!

It’s a beautiful day in the neighborhood to view spring flowers, but no time to smell flowers during pandemic mask wearing…