https://www.youtube.com/watch?v=-L0dIOxLhbk
With this month’s 50th anniversary of Harold and Maude (1971) and announcement of the upcoming film soundtrack release by Cat Stevens/Yusuf, I decided to revisit Harold and Maude through clinical social work lens.
“Clinical social work is a specialty practice area of social work which focuses on the assessment, diagnosis, treatment, and prevention of mental illness, emotional, and other behavioral disturbances.” –National Association of Social Workers
Hey, what about focus on whole person in environment?! Though my job description involves clinical social work, I continue to view myself foremost as a gerontologist working with older clients (and their families/significant others) to understand what’s important for their quality of life and helping them navigate the dysfunctional long-term care system.
As a first
year MSW student (back in pre-pandemic times), I chose Harold and Maude, a funny and touching film celebrating an intergenerational relationship, in a DSM (Diagnostic and Statistical
Manual of Mental Disorders) course assignment to conduct a biopsychosocial
analysis of a film character. This clinical lens nearly ruined my
film watching experience, but I will not let clinical social work ruin my
affinity for working with older adults!!!
Harold
and Maude: Clinical Analysis of Harold and his Mother
Based
on the character/characters, provide a biopsychosocial analysis of the
character/characters of the film you chose.
Harold and Maude showed only a week in
the life of Harold, revealing little information about his earlier life, and
even less about Harold’s mother, Mrs. Chasen.
My analysis will focus mostly on Harold, and a bit about his mother who
was influential in Harold’s development before he met Maude.
A. What is the diagnosis of the main character/characters and what type of symptomatology was present that led you to come to this assessment? When coding the diagnosis, use the ICD-10 coding. If there was not a diagnosis, you can use a provisional diagnosis and explain why you chose a provisional.
Prior
to meeting Maude, Harold’s diagnosis
appeared to be other specified depressive disorder, depressive episode with
insufficient symptoms (F32.8), as indicated by his depressed affect and at
least one of the other eight symptoms of a major depressive episode associated
with clinically significant distress or impairment that persisted for at least
two weeks: recurrent thoughts of death (American Psychiatric Association, 2013,
pp. 183-184). Harold appeared obsessed
with death – attending funerals of strangers, driving a hearse, and staging at
least 15 suicides.
Harold’s domineering socialite mother, Mrs. Chasen, appeared to have a diagnosis of narcissistic personality disorder (F60.81), as indicated by her pervasive pattern of grandiosity, need for admiration, and lack of empathy; she had a grandiose sense of self-importance, believing that she is superior and should associate with other high-status people, had a sense of entitlement, lacked empathy, and showed arrogant behaviors or attitudes (American Psychiatric Association, 2013, pp. 669-670). She appeared mostly insensitive to the needs of her son, responding to his staged suicides with indifference, like rolling her eyes while swimming past Harold when he was floating face down in their pool, and remarks such as “be a little more vivacious” when Harold was gagging with a noose around his neck hanging from the ceiling in their home. She appeared self-absorbed with social events and maintaining social status, including controlling her son’s. After finding a computer dating service that “screens out the fat and ugly, so it’s obviously a firm of high standards,” she proceeded to complete the dating questionnaire with her own answers. She unilaterally replaced Harold’s beloved hearse with a sportscar, which she perceived as more befitting for her young son.
B. If you were using a specific assessment or screening tool, which would you use to elaborate on your assessment?
For
baseline screening, I would use PHQ-9 for Harold’s depression and P4 for
suicidality. Prior to meeting Maude, Harold could self-report affirmatively to the
following two PHQ-9 items, which support other depressive disorder: Feeling down, depressed, or hopeless; and Thoughts that you would be better off dead,
or thoughts of hurting yourself. Harold expressed suicidal ideation and
staged fake suicides not for his mother’s “benefit,” as he told his
psychiatrist, but perhaps for his benefit to dramatically re-create “death” to
gain his mother’s attention/affection (see F below). While Harold had past suicide attempts and
plan for suicide, preventive factors outweighed his probability of carrying out
suicide. The fact that Harold kept himself alive through his staged suicides
suggests that he was seeking more from his existence than his basic
physiological and safety needs provided by his affluent mother, such as seeking
to satisfy higher needs of belonging, esteem and self-actualization. Harold appeared
obsessed with death as an escape from his stultifying existence controlled
by his emotionally cold mother.
Screening and assessing Harold’s mother for narcissistic personality disorder using her self-report is challenging because of the subject’s limited self-awareness and purposeful deception. Instead, I would make a clinical judgment based on observations and DSM-5 criteria.
C. If substance use was part of the coping mechanism for the character/characters, how did it play a role with their overall symptoms?
Maude encouraged Harold to consume “after-dinner liquor” (alcohol
= depressant) and smoke hookah (nicotine = both depressant and stimulant) in
the context of sharing an activity, though straitlaced Harold said he didn’t
drink and considered smoking a vice.
Maude seemed to market substance use as a coping mechanism to liberate
Harold from being “too moral,” thus getting cheated out of “too much life” so
he felt dead inside, or depressed.
Harold’s reluctance to partake in substance use likely alienated him
from social conformists, especially during the early 1970s when hookah was
popular and evidence of health dangers were not well-known at the time.

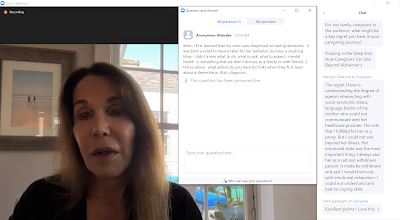
D. How would you engage with this individual/individuals in order to establish a strong therapeutic alliance?
To establish a strong therapeutic alliance with Harold, I
would use Carl Rogers’ person-centered approach of showing unconditional
positive regard for his well-being and empathic understanding through active
listening and creating a safe space for Harold to express himself. I would greet Harold with a warm smile, “Hi,
I’m Awe Some. How are you doing?” I would observe and listen to Harold’s
response. Then, I would offer, “Would
you like some water to drink?” This
introduction would set the tone for a safe, supportive environment by being
courteous and attentive to Harold’s needs as a person. Offering water demonstrates hospitality and
encourages Harold to freely talk without undue concern about thirst. Next, I would motion to a chair and offer,
“Would you like a seat?” Then, I would
try to sit at a 45-degree angle from Harold for eye contact while placed less
confrontational than directly in front of him.
This would be in contrast to Harold’s visits to his psychiatrist, who
were not seen exactly eye-to-eye:
side-by-side so they had to awkwardly turn their heads to face each
other, or Harold laying on the chaise staring at the ceiling and later
sleeping.
To meet Harold where he is, I would express my
condolences to Harold over Maude’s passing, and adopt a cultural humility
approach—assume nothing, be curious and interested in learning about Harold’s
uniqueness in all its complexity. As a
guide, I would use the Cultural Formulation Interview (American Psychiatric
Association, 2013, pp. 752-754). Since
individuals respond to loss in their own way, I would seek to understand
Harold’s perspective and ask him how he is feeling about Maude’s death and his
purpose in seeking therapy: “What brings you here today?” This open-ended question
would allow Harold to respond with his own agenda, empowering him with autonomy
and choice. To respect his
self-determination, I would communicate as a facilitator by suggestion, instead
of direction, using motivational interviewing’s OARS: Open-ended questions, Affirmation,
Reflection, Summaries. This approach is
in contrast to Harold’s condescending psychiatrist (who lectured Harold, “I
find you a very interesting case, but this reluctance on your part is
detrimental to the psychoanalytic process”) and judgmental priest (who
condemned Harold’s proposed marriage to Maude, ignoring their spiritual
relationship and expressing disgust as he imagined their physical intercourse
without goal of procreation—Harold’s “firm, young body co-mingling with” Maude’s
“withered flesh, sagging breasts, and flabby buttocks”).
Maude appears to be the only person who connected with
Harold in any meaningful and reciprocal way, so seeing how Maude was able to
draw out Harold, I would be authentic, use gentle humor and questioning as well
as empathic listening to provide space for Harold to express himself including
reminiscing on Maude’s influence and even making a list of Maude’s most
memorable quotes for reference to feel better (see strengths and healthy coping
mechanisms under G below). I would
encourage Harold, if ready, to continue exploring to find out what he wants,
including sources of inspiration, joy, and purpose. This approach is based on a strengths model focused on his existing resources. Finally, I would validate Harold’s
strengths (see G below).
I would be cautious in engaging with Harold’s mother because people with narcissistic personality disorder may lack insight so they may deny having any personality disorder. Mrs. Chasen appeared content with maintaining her status quo—a life of social events—rather than seeking to change herself, learn empathy through therapy, and develop a closer relationship with her son.
E. How did environmental factors play a role with the assessment? Describe how demographics, gender-sexuality, culture, housing, education, income, spirituality, biology and social support in general contributed to their psychosocial stressors and strengths?
Harold appeared to be an adult teen or twentysomething single
heterosexual white male from a socio-economically privileged family
background. He attended boarding school
and lived with his socialite mother in a mansion in the San Francisco Bay Area,
which may have restricted his socialization to this social class and
conservative lifestyle. He appeared to
be an only child, isolated from peers, and surrounded by, but mostly ignored
by, adults in his home (mother and servants) and at funerals of strangers. Mrs. Chasen, Uncle Victor and psychiatrist
provided nominal social support to Harold.
According to his mother, Harold was a “delicate child”
prone to illness and his father had a “sense of the absurd” such as getting
arrested for swimming in the nude. Harold’s
domineering mother decided after “an idle happy life of a child,” it was time
for Harold to take on “adult responsibilities” and marry from a sense of noblesse
oblige.
Harold appeared clean-cut, ectomorphic and neatly dressed
in blazer, dress pants and mostly oxford shirt with tie or turtleneck. He was polite, introverted, quiet and
sometimes morose. His attitude was
respectful and cooperative, following the rules and keeping appointments with
dates—though with some rebellion, such as pulling pranks (self-immolation,
chopping fake hand, and hara-kiri) to sabotage his mother’s plans for
him to take on “adult responsibilities” like meeting prospective suitors
through a computer dating service and enlisting him in the Army through Uncle
Victor. He also repurposed the sportscar
his mother bought him into a hearse. His
rebellions were evidence of his intelligence, particularly his cleverness in
staging realistic suicides and mechanical ability with redesigning the
sportscar into a hearse.
Harold presented wide-eyed, alert and oriented x3. He was reticent, spoke in measured words,
monotone, articulate manner. His mood
was mostly calm and euthymic, but uplifted in the presence of energetic and
refreshing Maude who befriended him a week before she took her own life. Even Harold’s pale skin tone acquired some
coloring after meeting Maude. His affect
was mostly flat, detached. He appeared
to be going through the motions of what his repressive mother expected of him,
a stifling situation that was probably “killing him” deep down inside. He was unemployed, seemingly lacking purpose
or meaning in his life. When asked by
his psychiatrist what he did for enjoyment, Harold replied he attended
funerals; and he visited junkyards and observed demolitions.
Harold’s attendance at funerals might suggest yearning
for spirituality, something deeper than the superficiality of his fleeting
physically comfortable existence. (Think
Ecclesiastes 7:2: “It
is better to go to the house of mourning, … for that
is the end of all men; and the living will lay it to his heart.”) At funerals, there is reflection on the
deceased person that gives meaning to life and inspiration for the living on
how they would like to be remembered.
Harold’s mother appeared to be a WASPy, middle-aged widow, svelte and attractive, with perfectly coiffed hair and elegant dress. She was self-absorbed, defensive, alert, oriented x3. She was talkative; spoke fast, strong and clear. Her mood and affect were detached; her thoughts appeared related to maintaining her social standing. She expressed concern for her son by helping him find a wife and vocation in the Army, but otherwise she appeared self-satisfied.
F. Was there a history trauma/oppression that played a role in your overall assessment?
Though not explicitly addressed in the film, it’s possible that Harold’s depression—appearance of being socially withdrawn, emotionally restricted and numb and lack of interest in anything outside of death—could be related to a history of trauma from the loss of attachment to a supportive parent figure. Mrs. Chasen’s apparent indifference might be a source of trauma/oppression as Harold related that “I haven’t lived, but I’ve died a few times”: while in his boarding school’s chemistry lab, he accidentally caused an explosion leading police to assume he was killed so they informed his mother who reacted by collapsing into the arms of police; this was when Harold decided he “enjoyed being dead,” crying for his mother’s attention through staged suicides. At times, Harold’s mother appeared to control Harold’s life: eating beets, finding a wife and vocation, buying a car, etc. Harold did not mention his father, whose role in Harold’s life is unknown.
G. What type of strengths and healthy coping mechanisms did you find in the character/characters?
Harold’s strengths are his personal qualities of being earnest, open-minded, empathic with a strong sense of morality; for example, he respectfully told Maude that driving off with strangers’ cars was “upsetting people, I don’t know if that’s right.” Harold was open to forming a friendship with a more experienced older woman Maude, and learning her life’s lessons on how to live more fully in the process, so adaptation was his healthy coping mechanism. In contrast to Harold’s escapism, vivacious Maude embraced life – attending funerals as a celebration of life – and showed him life is worth living and savoring with all senses (playing banjo for listening ears, painting for seeing eyes, odorific for smelling nose, etc.), nature (saving suffocating tree from city street and replanting in forest) and adrenaline-inducing experiences (though Harold questioned Maude’s stealing and reckless driving). As an accomplice to Maude’s pranks, Harold began to consider her advice to take chances in life and get outside of himself to “look for new experiences” and “can’t let the world judge you too much.” Maude did not appear tied to social conventions but appeared content to live a hedonistic life on her own idiosyncratic terms. Reflecting on this might help Harold recognize that being true to oneself like Maude might be an alternative to seeking attention from his phony mother.

Just as Maude liberated the canaries from cages, we see
Harold begin to break out of his existential crisis, becoming more expressive
and open to new life experiences. If
Maude could survive the Holocaust (not mentioned, but suggested by her numbered
tattoo in the scene when Harold holds her hand) and take back control of her
own life, then Harold also could survive and take control of his own life,
liberated from the strictures of his controlling mother.
In her irreverently charming manner, Maude used cognitive
behavioral therapy to change Harold’s outlook and attitude, opening up
possibilities that helped him cope with his depression. When Maude asked him what kind of flower he
would like to be and Harold pointed to a bed of daisies explaining “because
they’re all alike,” Maude taught him to pay closer attention to observable differences,
a metaphor for how each person is unique; and how much of the world’s sorrow
come from people who are unique but allowed themselves to be treated
otherwise. Another example was when
Harold faced despair over being enlisted in the U.S. Army, Harold partnered
with Maude to make fun of the situation with Harold faking his passion for
killing and feud with pacifist Maude, which ultimately persuaded Uncle Victor
that Harold was not of sound mind for Army service.
Harold demonstrated strength in ignoring the superficiality of his mother, Uncle Victor, his psychiatrist and the priest who mainly noticed the age gap between Harold and Maude. When Harold declared his love for dying Maude while riding in the ambulance, she encouraged him, “Go love some more!” Harold was able to cope with death, which he did not deny or fear, and Maude helped him to accept death by viewing burials and birth as part of the “great circle of life.” Maude hinted that she planned to end her life on her 80th birthday on several occasions, including their first meeting (“80 years old, good time to move on, don’t you think?”) and advising not to get attached because “here today, gone tomorrow!”

Near the end of the film, we see the change in Harold,
who had been nonchalantly faking suicides, but then reacted with real concern
to Maude’s real suicide by rushing her to the hospital. After Maude’s death, we see Harold speeding
in his hearse that plunges off a cliff, which is another fake suicide as we see
Harold on the cliff playing the banjo while skipping about like his mentor
Maude who lived life joyfully. Within
just one week, Harold transformed to be more like Maude with a changed
perspective that is life-affirming, a strength that will help him cope as he
moves forward, appreciating one day at a time, living life to the fullest.
Harold evolved from a depressed young man, perplexed about existence, into a
stronger, more confident man with greater peace of mind.
Harold’s mother had strength to survive widowhood and be a single parent to an only child who seemed to exasperate her with staged suicides. She coped by referring her son to male caricatures like the banal psychiatrist and militant Uncle Victor. She also used the strength of her socio-economic privilege to move ahead in the world, ignoring most obstacles, which seemed to suit her.
Intergenerational relationships
For my assignment, I avoided looking for DSM-5 diagnosis in Maude character. After all, Maude’s appeal is her nonconformity/anti-Establishment stance, which is pathologized under DSM. Instead, I chose to focus on the value of the intergenerational relationship: Maude as wise mentor to younger, less experienced Harold, who has been oppressed by authoritarian figures like his mother, priest, psychiatrist, Uncle Victor (like Uncle Sam recruiter for US Army) trying to “cure” his eccentricity instead of embracing it like Maude.
Media reports
on mutuality of intergenerational relationships:
· “88-year-old graduates college alongside his 23-year-old granddaughter”: Rene Niera, terminally ill and in hospice care, achieved lifetime goal of earning economics degree, begun in 1950s and resumed while studying alongside his granddaughter at community college and then University of Texas (Today, Dec. 23, 2021).
· “Roommates and best friends: She’s 101, he’s 78”: Martin Jacobs was 55 when his mother introduced him to 80-year-old Jean Milgram in 1999, bonding over mutual interests (J Weekly, Dec. 21, 2021).
· “Teaching university students to be ‘age-conscious’ could help address our eldercare crisis”: The gold standard of intergenerational learning is through service learning, when both (younger) students and older people collaborate on an shared activity (The Conversation, Nov. 18, 2021).

Interesting observation: 79-year-old Maude (played by then 74-year-old Ruth Gordon) had same brown hair coloring like much younger Harold (played by then 23-year-old Bud Cort, almost same age as Cat Stevens).
2021: “Year of gray hair”
“Before gray hair you should rise up, and you must show honor to an older man, and you must be in fear of your God.”—Leviticus 19:32
If Leviticus had included honor to an older woman (and not just older man!), perhaps older women wouldn’t wait for COVID-19 pandemic lockdown to accelerate granny hair trend? (Or use Bible translations that refer to the elderly, old person, older people, the old, the aged, etc.)
Vogue (not quite an authority like the Bible) proclaimed 2021 “The Year of Gray Hair” with women embracing their natural changing hair color during COVID pandemic. Several actresses wondered why can’t women be more like men who already “embrace” beautiful/exquisite gray hair?
I feel better like this. Honestly, it’s exhausting to have to be something that you no longer are. I was finally like, “You know what? I’m not young. And I’m okay with that …I was looking at pictures of men, where they’re just their age, they’re normal, and we think they’re beautiful. I thought, okay, I may age and I want to be beautiful. So that’s where I got my “manspiration.”--Andie MacDowell (age 63), Interview (Oct. 19, 2021)
There’s so much misogynist chatter in response to us that would never. Happen. About. A. Man…Does she have gray hair?’ I’m sitting with Andy Cohen, and he has a full head of gray hair, and he’s exquisite. Why is it okay for him?... It almost feels as if people don’t want us to be perfectly okay with where we are …whether we choose to age naturally and not look perfect, or whether you do something if that makes you feel better. I know what I look like. I have no choice. What am I going to do about it? Stop aging? Disappear?—Sarah Jessica Parker (age 56), Vogue (Dec. 2021)
Today’s
announcement of Betty White’s death at age 99 made me think I want to age like
she did, more about her character than appearance.
Don’t try to be young. Just open your mind. Stay interested in stuff. There are so many things I won’t live long enough to find out about, but I’m still curious about them.—Betty White (1922-2021), “Betty White, TV’s Golden Girl, dies at 99,” Associated Press (Dec. 31, 2021)

https://www.youtube.com/watch?v=D9_wIu8ePxs&t=4s
Judy Chicago, 82-year-old feminist artist with white/purple hair, has her own retrospective show at de Young Museum. She noted the female experience has been marginalized, so her work has been to intervene to “move art world where everybody’s voice matters.”

“What
if women ruled the world?... Would old women be revered?”
--Judy Chicago, The Female Divine (2020)
In The Female Divine (2020), Judy collaborated with all-women Chanakya School of Craft (Mumbai, India), which executed 11 velvet banners of hand embroidery and brocade, each asking rhetorical questions. More controversially, Judy’s smoke bomb show at Golden Gate Park was viewed as “radical hypocrisy.”
Health is social

Oh my, omicron variant surge is here! Increasing COVID-19 cases and hospitalizations trending so another pause on home visits with clients, and return of universal indoor masking (though disappointed SF DPH adopted controversial CDC guidelines for shortening isolation time). According to CDC, 1 in every 100 older adults in USA has died of COVID-19, and more than 75% of COVID-19 deaths were people age 65+.
Wonder when this world will embrace collective care (end vaccine apartheid!) rather than self-care?
Here we go again, say Katherine
J. Wu, Ed Yong and Sarah Zhang, in “Omicron Is Our Past Pandemic Mistakes on Fast-Forward” (The Atlantic, Dec. 23, 2021):
1. We rush to dismiss it as “mild.”…but
more transmissible virus can spread so aggressively that it ultimately causes more
hospitalizations and deaths.
2. We treat vaccines as all-or-nothing
shields against infection.
3. We still try to use testing as a
one-stop solution…yet they need to be accessible, reliable and fast…COVID cases
overwhelming USA’s frayed testing infrastructure.
4. We pretend the virus won’t be
everywhere soon.
5. We fail to prioritize the most
vulnerable groups…like older adults!
6. We let health-care workers bear the
pandemic’s brunt.
According to Ed Yong, public health needs to go back to its 19th century progressive era roots of addressing societal weaknesses to prevent spread of epidemics (social solution for collective problem) v. relying on 20th century germ theory that focuses on pathogens/vaccine solution.
“…public
health began to treat people as if they lived in a social vacuum. Epidemiologists
now searched for “risk factors,” such as inactivity and alcohol consumption,
that made individuals more vulnerable to disease and designed health-promotion
campaigns that exhorted people to change their behaviors, tying health to
willpower in a way that persists today…
The
biomedical view of health still dominates, as evidenced by the Biden
administration’s focus on vaccines at the expense of masks, rapid tests, and
other “nonpharmaceutical interventions.” Public health has often been represented
by leaders with backgrounds primarily in clinical medicine, who have repeatedly
cast the pandemic in individualist terms: “Your health is in your own hands,” said
the CDC’s director, Rochelle Walensky, in May, after announcing that the
vaccinated could abandon indoor masking…
If
anything, the pandemic has proved what public health’s practitioners understood
well in the late 19th and early 20th century: how important the social side of
health is. People can’t isolate themselves if they work low-income jobs with no
paid sick leave, or if they live in crowded housing or prisons. They can’t
access vaccines if they have no nearby pharmacies, no public transportation, or
no relationships with primary-care providers. They can’t benefit from effective
new drugs if they have no insurance. In earlier incarnations, public health
might have been in the thick of these problems, but in its current state, it
lacks the resources, mandate, and sometimes even willingness to address them.”
—Ed Yong, “How Public Health Took Part in Its Own Downfall: The field’s future lies in reclaiming parts of its past that it willingly abandoned," The Atlantic (Oct. 23, 2021)
Sounds
awfully like medicalization of social work/clinical social work focused on
professional self-care and pathologizing individual client instead of
advocating to strengthen social safety net (universal basic income to lift
people out of poverty, universal healthcare/long-term care system, paid sick
leave, etc.). Need to put social back into social work!

https://www.youtube.com/watch?v=0QpjR6-Uuks
Yusuf Islam/Cat Stevens sounds and looks cool with gray hair at age 73!
Now
I've been cryin' lately
Thinkin' about the world as it is
Why must we go on hatin'?
Why can't we live in bliss?
'Cause out on the edge of darkness
There rides a peace train
Oh, peace train take this country
Come take me home again
--Cat Stevens, “Peace Train” (1971)